Male Physiology: The Hidden Psychology of the Prostate
Introduction and Anatomical Location
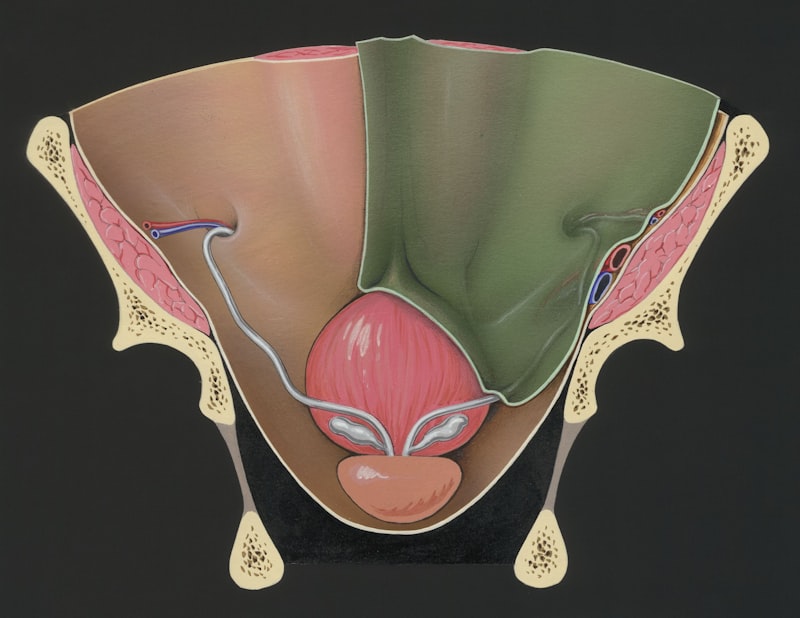
The prostate gland is a crucial accessory sex gland found exclusively in the male reproductive system. Anatomically, it is a dense, fibromuscular, and glandular organ generally described as being chestnut-shaped, though its precise morphology can vary significantly among individuals. This gland is strategically located in the pelvis, situated immediately inferior to the urinary bladder and superior to the urogenital diaphragm. Its unique positioning means it completely surrounds the initial portion of the urethra, known as the prostatic urethra, through which urine and seminal fluid must pass. This close relationship between the prostate and the urinary outflow tract is central to understanding the symptoms associated with many common prostatic diseases, especially those related to aging and enlargement of the gland itself.
Understanding the internal structure of the prostate is essential for comprehending its function and pathology. The prostate is encased within a fibrous capsule and is often divided anatomically into specific zones, a classification system developed by McNeal that is highly relevant in clinical practice. The primary zones include the peripheral zone, which constitutes the largest volume of the gland (about 70%) and is the most common site for prostate cancer development. The central zone surrounds the ejaculatory ducts and makes up approximately 25% of the glandular tissue. Crucially, the transitional zone, though small in youth (about 5%), is the region that undergoes significant hyperplastic growth later in life, leading to Benign Prostatic Hyperplasia (BPH). Finally, the anterior fibromuscular stroma is non-glandular tissue composed mostly of muscle and connective tissue, lying anteriorly.
The prostate receives its blood supply primarily from the inferior vesical artery, with venous drainage forming the extensive prostatic venous plexus, which eventually connects to the internal iliac veins. Innervation is supplied by the inferior hypogastric plexus, playing a vital role in regulating glandular secretion and the smooth muscle contractions necessary for ejaculation. The prostate’s precise location, nestled between the bladder neck and the external urethral sphincter, necessitates careful surgical and diagnostic approaches, as damage to surrounding structures, particularly the nerves responsible for erectile function, remains a significant clinical concern during interventions like prostatectomy.
Physiological Role and Function
The primary physiological role of the prostate gland is the production and secretion of prostatic fluid, a critical component of seminal fluid, which is the vehicle that transports sperm during ejaculation. Although the fluid itself accounts for only about 20% to 30% of the total volume of semen, its chemical composition is fundamental to ensuring the viability and motility of spermatozoa. This fluid is designed to optimize the environment for sperm survival, particularly after deposition into the relatively hostile acidic environment of the female reproductive tract. The timing of the fluid secretion is synchronized through a complex neurophysiological cascade that occurs during sexual arousal and culminates in the rhythmic contractions of the smooth muscle within the prostate gland itself, propelling the fluid into the prostatic urethra where it mixes with sperm and fluid from the seminal vesicles.
Beyond simply contributing volume, the prostatic secretions activate sperm, helping them transition from a relatively quiescent state within the male ducts to a highly motile state required for fertilization. The fluid ensures that sperm are properly nourished and protected during their journey. Furthermore, the muscular tissue surrounding the prostatic urethra plays a mechanical role during ejaculation. Contractions of the smooth muscle tissue prevent the retrograde flow of semen into the bladder—a condition known as retrograde ejaculation—while simultaneously generating the pressure needed to expel the seminal mixture forward through the penis. This dual function of glandular secretion and muscular coordination highlights the prostate’s essential role in human fertility and reproductive success.
The prostate’s contribution is intricately linked with other accessory glands. While the seminal vesicles contribute the majority of the volume, rich in fructose (the primary energy source for sperm), the prostate provides the necessary enzymes and buffers. This collaborative effort ensures the complete functional integrity of the semen. Without the crucial components provided by the prostate, the semen would lack the necessary chemical characteristics to maintain sperm viability and neutralize environmental threats, thereby severely compromising the likelihood of successful fertilization. The sophisticated regulatory mechanisms governing the prostate’s function underscore its indispensable nature in reproductive physiology.
Composition of Prostatic Fluid
Prostatic fluid is characteristically thin, milky, and slightly opaque in appearance due to its complex mixture of proteins, enzymes, minerals, and small organic molecules. Importantly, the fluid is slightly alkaline, possessing a pH typically ranging between 7.2 and 7.4. This alkaline nature is critical because it acts as a buffer against the natural acidity of the vaginal environment, which is maintained by lactobacilli and is typically around pH 3.5 to 4.5. If the semen were not buffered, the spermatozoa would be rapidly immobilized and destroyed upon entry into the vagina, thus the alkalinity provided by the prostate is a key protective mechanism ensuring the spermatozoa have a chance to reach the ovum.
Among the most studied and clinically relevant components of prostatic fluid is Prostate-Specific Antigen (PSA). PSA is a serine protease enzyme that functions to liquefy the seminal coagulum formed shortly after ejaculation, a process vital for freeing the sperm to begin their upward migration through the female reproductive tract. While PSA is essential for reproductive function, its presence in the bloodstream is used extensively as a clinical marker for screening and monitoring prostate health, particularly concerning prostate cancer and BPH. High levels of circulating PSA, while not diagnostic of cancer alone, often prompt further investigation due to the potential association with prostatic pathology.
Other significant constituents include various molecules that contribute to prostatic function and health. These include high concentrations of citric acid (citrate), which helps maintain osmotic balance and potentially plays a role in zinc chelation; acid phosphatase, another enzyme that assists in breaking down components for sperm nutrition; and significant amounts of zinc. Zinc plays a vital role in stabilizing the DNA chromatin in the sperm head and is thought to possess antibacterial properties, contributing to the defense against urinary tract infections and prostatitis. The careful balance of these components, regulated by hormonal signals, dictates the overall health and functionality of the gland, making the prostatic fluid a finely tuned biochemical medium.
Regulation and Hormonal Influence
The growth, development, and secretory activity of the prostate gland are heavily dependent upon a complex interplay of hormones, primarily the androgens. The prostate is an classic example of an androgen-dependent organ, meaning that its structure and function are maintained by male sex hormones. The primary circulating androgen is testosterone, which is produced predominantly by the testes. However, testosterone itself is not the most potent androgen acting within the prostate; rather, it serves as a precursor that must be converted locally within the prostatic cells to its more active metabolite.
This critical conversion process is mediated by the enzyme 5-alpha reductase, which transforms testosterone into dihydrotestosterone (DHT). DHT is significantly more potent than testosterone and binds tightly to androgen receptors within the prostatic stromal and epithelial cells. This binding stimulates cell proliferation and promotes the secretory functions of the gland. The essential role of DHT is evidenced clinically by the effectiveness of 5-alpha reductase inhibitors (5-ARIs), such as finasteride, which block this conversion pathway. These medications are used successfully to treat BPH by reducing the level of DHT, thereby causing the prostate to shrink and alleviating associated urinary symptoms.
Hormonal regulation is also intrinsically linked to the development of prostate diseases. For instance, the age-related shifts in androgen and estrogen balance are considered major contributors to the pathogenesis of BPH. While testosterone levels may decrease slightly with age, the ratio of DHT to testosterone, and the local accumulation of DHT, appear to drive the hyperplastic growth in the transitional zone. Furthermore, the hormonal dependency of the prostate is central to the treatment of advanced prostate cancer; androgen deprivation therapy (ADT), which aims to reduce circulating levels of androgens, remains a cornerstone treatment strategy for slowing tumor growth, highlighting the prostate’s lifelong reliance on hormonal signaling for both health and disease progression.
Benign Prostatic Hyperplasia (BPH)
Benign Prostatic Hyperplasia, commonly referred to as BPH, is perhaps the most prevalent prostatic condition, affecting the majority of men as they age. It involves the non-malignant, excessive growth of stromal and epithelial cells within the prostate, specifically concentrating in the periurethral region, or the transitional zone. This growth leads to an overall increase in the size of the gland, which subsequently compresses the prostatic urethra. Because BPH is fundamentally driven by age-related hormonal changes, particularly the sustained presence of DHT, its incidence increases sharply after the age of 50, becoming almost ubiquitous in octogenarians, though only a fraction of affected men develop clinically bothersome symptoms requiring intervention.
The clinical manifestation of BPH involves a spectrum of symptoms collectively known as Lower Urinary Tract Symptoms (LUTS). These symptoms are broadly categorized into two groups: voiding (obstructive) symptoms and storage (irritative) symptoms. Voiding symptoms result directly from the mechanical obstruction of the urethra and include urinary hesitancy (difficulty starting the stream), a weak or interrupted stream, straining to void, and incomplete bladder emptying, which can lead to retention. Storage symptoms, conversely, often relate to secondary changes in the bladder wall attempting to overcome the obstruction, manifesting as urinary frequency, urgency, and nocturia (waking up multiple times at night to urinate). These symptoms significantly impact the quality of life, ranging from mild annoyance to severe debilitating discomfort.
Management of BPH ranges from conservative measures to surgical intervention, depending on symptom severity and the presence of complications. Initial treatments often involve watchful waiting for mild symptoms, coupled with lifestyle modifications. Pharmacological therapies are highly effective for moderate symptoms, primarily utilizing two classes of drugs: alpha-adrenergic blockers (e.g., tamsulosin), which relax the smooth muscles in the prostate and bladder neck to improve urine flow; and 5-alpha reductase inhibitors (5-ARIs), which reduce the volume of the prostate gland over time by blocking DHT production. For cases refractory to medication, or those complicated by recurrent urinary retention, kidney damage, or persistent gross hematuria, surgical procedures like Transurethral Resection of the Prostate (TURP) remain the gold standard for removing the obstructive tissue.
Prostatitis (Inflammation)
Prostatitis refers to the inflammation of the prostate gland, a condition that is often complex to diagnose and treat due to its varied etiologies and symptom presentation. Prostatitis is generally classified into four categories defined by the National Institutes of Health (NIH) consensus classification system. Type I is acute bacterial prostatitis, a severe infection characterized by sudden onset, high fever, chills, and significant painful urinary symptoms. Type II is chronic bacterial prostatitis, which involves recurrent urinary tract infections caused by persistent bacterial infection within the prostate, often presenting with intermittent symptoms over a long period. Types III (Chronic Pelvic Pain Syndrome, CPPS) and IV (asymptomatic inflammatory prostatitis) are much more common and less understood, particularly Type III, which involves chronic pain in the pelvic region without clear evidence of ongoing bacterial infection.
Acute bacterial prostatitis (Type I) is a medical emergency requiring prompt treatment, typically involving broad-spectrum antibiotics that can adequately penetrate the prostatic tissue, such as fluoroquinolones. If left untreated, the infection can potentially lead to life-threatening sepsis or localized abscess formation. Chronic bacterial prostatitis (Type II), while less severe acutely, is challenging due to the need for prolonged antibiotic courses (often 4 to 12 weeks) to eradicate bacteria sequestered deep within the glandular tissue, preventing recurrence. Diagnosis often requires culturing expressed prostatic secretions or urine samples taken after prostatic massage to identify the causative organism.
Chronic Pelvic Pain Syndrome (CPPS, Type III), which accounts for over 90% of all prostatitis diagnoses, presents the greatest diagnostic and therapeutic challenge. Patients experience persistent pelvic pain, often localized to the perineum, scrotum, or lower back, frequently accompanied by urinary frequency and painful ejaculation. This syndrome is often non-infectious, involving potential mechanisms such as autoimmune responses, chemical irritation, neurological dysfunction, or pelvic floor muscle tension. Treatment for CPPS is highly individualized and multimodal, involving lifestyle changes, pain management, alpha-blockers, and sometimes physical therapy aimed at relaxing the pelvic musculature, underscoring the complexity of managing prostatic inflammation that is not purely infectious in nature.
Prostate Cancer: Epidemiology and Risk Factors
Prostate cancer is one of the most significant health concerns for men globally, being the second most frequently diagnosed cancer in males and a leading cause of cancer-related death. The disease typically originates in the glandular epithelial cells, with the vast majority of cases (approximately 70% to 80%) arising in the peripheral zone of the gland, making it often palpable during a Digital Rectal Exam (DRE) in its early stages. The clinical course of prostate cancer is highly variable; it can range from indolent, slow-growing tumors that may never cause clinical harm, to aggressive malignancies that rapidly metastasize, particularly to the bones and lymph nodes.
Multiple factors contribute to the risk profile for developing prostate cancer, with age being the single most powerful determinant. The incidence rises exponentially after the age of 50, making regular screening crucial for older men. Genetics and family history also play a significant role; men with a first-degree relative (father or brother) diagnosed with prostate cancer have a twofold to threefold increased risk. This risk is even higher if the relative was diagnosed at a younger age. Furthermore, specific inherited gene mutations, such as those in the BRCA1 and BRCA2 genes, which are traditionally associated with breast and ovarian cancers, also confer a substantial increase in prostate cancer risk, often correlating with more aggressive disease presentation.
Another major non-modifiable risk factor is ethnicity. Men of African descent consistently demonstrate the highest incidence rates of prostate cancer worldwide, often presenting with the disease earlier and experiencing higher mortality rates compared to Caucasian or Asian populations. While lifestyle and dietary factors are continuously researched—with high consumption of red meat, obesity, and lack of exercise potentially increasing risk—the primary risk stratification remains centered on age, family history, and ethnic background. Due to the high prevalence and potential aggressiveness of the disease, the common advice remains highly pertinent: “Every male over the age of 50 should have his prostate gland checked regularly.”
Diagnostic Procedures and Screening
Early detection of potentially aggressive prostate cancer is achieved through screening, which typically involves a combination of two primary tests. The first is the Digital Rectal Exam (DRE), where a physician manually examines the prostate through the rectal wall to assess its size, symmetry, and texture, looking for nodules, hardness, or irregularities that might indicate malignancy, particularly since most cancers arise in the posterior-facing peripheral zone. The second, and more common screening tool, is the blood test measuring serum levels of Prostate-Specific Antigen (PSA). While elevated PSA is not specific to cancer—it can also be raised by BPH, prostatitis, or recent ejaculation—a persistently rising or abnormally high PSA level serves as an important red flag that warrants further diagnostic investigation.
Screening guidelines vary among medical organizations but generally recommend that discussions about screening begin around age 50 for men of average risk. For men at higher risk, such as those with a strong family history or men of African descent, screening discussions often commence earlier, around age 40 to 45. Decisions regarding screening must be made individually, considering the potential benefits of early detection versus the risks associated with false positives, unnecessary biopsies, and potential side effects from the treatment of indolent tumors (overdiagnosis and overtreatment).
If screening tests suggest potential malignancy (e.g., a suspicious DRE or persistently elevated PSA), further investigation is mandated. The definitive diagnostic procedure for prostate cancer remains the transrectal ultrasound-guided biopsy, where tissue samples are collected and examined pathologically. Increasingly, imaging modalities, especially multiparametric Magnetic Resonance Imaging (mpMRI), are being utilized prior to biopsy to identify suspicious areas more precisely, allowing for targeted biopsies and improving diagnostic accuracy. The collected tissue is then graded using the Gleason score, which assesses the aggressiveness of the tumor based on its cellular architecture, providing crucial information necessary for treatment planning and prognosis determination.