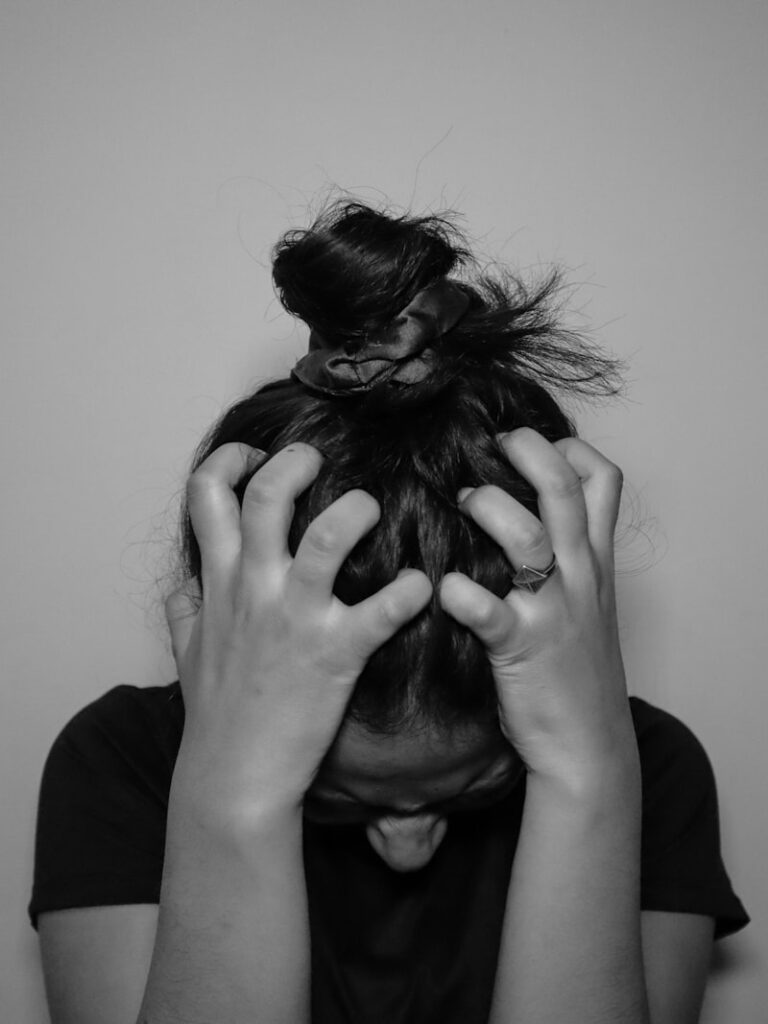
Stress Reaction: How Your Body Handles Pressure
Stress Reaction: Physiological and Psychological Effects The Core Definition of Stress Reaction The psychological concept of the Stress Reaction, often referred to as the stress response, is defined as the body’s non-specific physiological and psychological response to any demand made upon it, whether that demand is pleasant (eustress) or unpleasant (distress). It represents an intricate, […]

Emergency Theory: How Fear Powers Your Survival Instincts
Emergency Theory of Emotions The Core Definition of the Emergency Theory of Emotions The Emergency Theory of Emotions (ETE) is an influential and integrative model that fundamentally proposes that emotional experiences are not merely subjective feelings but are, first and foremost, rapid physiological and neural preparations designed to facilitate immediate survival. This theory asserts that […]
Adrenergic System: The Biology of Your Fight or Flight
The Adrenergic System The Adrenergic System: An Overview The adrenergic system stands as a pivotal regulatory network within the human body, intricately orchestrating a vast array of physiological functions, most notably in neurotransmission and crucial metabolic processes. It serves as a rapid response mechanism, allowing the body to adapt to various internal and external stimuli, […]
Biological Stress: How Your Body Handles the Pressure
Biological Stress Stress is an undeniable and pervasive aspect of human existence, influencing individuals across all walks of life. The manner in which a person perceives and responds to demanding situations holds profound implications for their overall physical and mental well-being. At its most fundamental level, biological stress represents the intricate physiological and psychological reactions […]
CANNON, WALTER BRADFORD (1871-1945)
Early Life and Education Walter Bradford Cannon (1871-1945) was an exceptionally influential American physiologist whose work revolutionized the understanding of bodily regulation, stress, and emotion. Born on October 19, 1871, in Prairie du Chien, Wisconsin, Cannon’s early life fostered a keen interest in the natural world and the mechanisms underlying biological function. His foundational education […]
NOREPINEPHRINE (Noradrenalin)
Introduction and Definition Norepinephrine, scientifically designated as L-Norepinephrine and widely known by its synonym noradrenaline (NA or NE), functions as both a crucial neurotransmitter within the nervous system and a vital hormone released by the adrenal medulla. It is a fundamental biogenic amine that plays an indispensable role in maintaining systemic homeostasis, particularly in mediating […]
ADRENERGIC REACTION
Defining the Adrenergic Reaction The Adrenergic Reaction refers specifically to the physiological responses elicited in target organs that receive innervation from the Sympathetic Nervous System (SNS) upon exposure to the endogenous catecholamines, epinephrine (adrenaline) and norepinephrine (noradrenaline). This reaction is fundamentally crucial for immediate survival, forming the core mechanism of the classic “fight-or-flight” response. It […]