Psychosexual Trauma: Healing the Impact of Early Wounds
Definition and Scope of Psychosexual Trauma Psychosexual trauma is defined as a severely damaging sexual experience, typically occurring during critical periods of psychosexual development in childhood or adolescence, that fundamentally alters the individual’s capacity for healthy sexual functioning and emotional regulation in later life. This type of trauma is distinguished by its direct assault on […]

Male Sexual Dysfunction: Understanding the Mind-Body Link
Definition and Scope of Male Sexual Disorder Male sexual disorder is an expansive and complex umbrella term used by clinicians and researchers to describe any persistent or recurrent impairment of sexual function or satisfaction experienced by a male individual. This definition covers a wide spectrum of conditions, ranging from issues in the desire phase to […]

Multiple Orgasm: The Psychology of Peak Pleasure
Introduction and Definition of Multiple Orgasm The concept of multiple orgasm refers to the physiological capability of an individual to experience a sequence of distinct, separate orgasmic peaks within a short timeframe, typically without entering a complete refractory period or the full resolution phase between experiences. This phenomenon is a subject of significant psychological and […]

Sexual Aids: The Psychology of Intimacy and Self-Discovery
Introduction and Definition The term dildo refers to a non-vibrating sexual aid typically designed to replicate or simulate the shape, size, and function of an erect human penis. Fundamentally defined as an artificial penis, the dildo serves as a primary tool for sexual gratification, masturbation, and various forms of partnered sexual activity. Within the broader […]
Preorgasmic: Understanding the Peak of Sexual Response
Introduction and the Dual Definitions of the Preorgasmic State The term preorgasmic carries significant weight within sexology and clinical psychology, representing two distinct yet interconnected phenomena related to human sexual response. Primarily, the term denotes the intense physiological and psychological state that immediately precedes the experience of orgasm, functioning as the peak of the plateau […]
Orgastic Potency: The Science of Total Emotional Release
Definition and Historical Context Orgastic potency is a highly specific concept within the fields of sexology and psychodynamics, primarily defined as the comprehensive capacity of an individual, regardless of biological sex, to achieve a total and satisfying organismic discharge during sexual activity. This definition transcends the mere achievement of climax; it emphasizes the ability to […]
Urolagnia: Understanding the Psychology of Paraphilia
Urolagnia Defined Urolagnia, derived from the Greek terms ouron (urine) and lagneia (lust or desire), is clinically categorized as a paraphilia characterized by persistent and intense carnal arousal associated with urine or the act of urination. This specific erotic fixation centers upon the excretory processes and the substance itself, serving as a primary or necessary […]

Female Sexual Arousal: Understanding the Intimacy Gap
Introduction and Definition of Female Sexual Arousal Disorder Female Sexual Arousal Disorder (FSAD) constitutes a significant clinical challenge characterized by a persistent or recurrent inability for a woman to achieve or sustain sufficient physiological or subjective sexual arousal until the completion of the sexual activity. This crucial phase, often referred to as the excitement phase […]

Ego-Dystonic Homosexuality: Resolving Inner Conflict
Introduction and Definition of Ego-Dystonic Homosexuality Ego-dystonic homosexuality refers to a specific clinical presentation where an individual experiences significant psychological distress and conflict regarding their own homosexual or bisexual orientation. Crucially, the disorder is not the sexual orientation itself, but rather the profound, unwanted dissonance between the individual’s experienced sexual attraction patterns and their consciously […]
Atypical Psychosexual Disorder: Beyond Clinical Labels
Introduction to Atypical Psychosexual Disorder The concept of Atypical Psychosexual Disorder serves as a critical placeholder within the nosology of sexual health, specifically designed to capture clinical presentations that defy neat categorization within established diagnostic frameworks. Originating prominently in the structure of the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR), […]

Sexual Dysfunction: Mastering Control for Better Intimacy
Clinical Definition and Diagnostic Criteria Premature Ejaculation (PE) is formally recognized as a persistent or recurrent pattern of ejaculation occurring during partnered sexual activity within approximately one minute following vaginal penetration and before the individual desires it. This condition represents a significant male sexual dysfunction characterized by a lack of voluntary control over the ejaculatory […]
Paragenital: Redefining Intimacy Beyond Reproduction
Introduction and Definition of Paragenital The term paragenital functions primarily as an adjective within clinical, psychological, and sociological texts, describing activities, methods, or conditions that correspond to carnal intercourse wherein the potential for conception is inhibited. This specific terminology is designed to categorize reproductive acts that, while involving typical genital function and coital behavior, are […]

Dyspareunia: Breaking the Cycle of Intimacy Pain
Definition and Clinical Significance Painful sexual intercourse, clinically termed dyspareunia, refers to persistent or recurrent genital pain that occurs before, during, or after sexual activity involving penetration. This condition represents a wide spectrum of discomfort, ranging from a mild burning sensation or irritation, often localized superficially near the vaginal opening, to intense, debilitating pain experienced […]
Sexuality Education: Guiding Healthy Human Development
Definition and Scope of Sex Education Sex education, often formally termed sexuality education, constitutes a structured and systematic course of instruction concerning human sexuality, reproductive processes, and sexual health. This pedagogical endeavor is fundamentally designed to be presented to young people in the school setting, although effective programming often involves community outreach and supportive family […]

Sex Therapy: Reclaiming Intimacy and Sexual Well-Being
Introduction and Definition of Sex Therapy Sex therapy is a specialized form of psychotherapy focused rigorously on the assessment and treatment of sexual disorders and dysfunctions. As a clinical practice, it utilizes specific techniques tailored to address a diverse range of conditions affecting sexual health, functioning, and satisfaction. These disorders may manifest across various dimensions, […]

Algolagnia: The Psychology of Pleasure Through Pain
Definition and Etymology of Algolagnia Algolagnia represents a specific category of sexual interest or paraphilia characterized by deriving sexual pleasure and arousal from experiencing pain, or from inflicting pain upon another individual. The term itself is derived from classical Greek, providing immediate insight into its core components. The first root, algos (ἄλγος), translates directly to […]

The Squeeze Technique: Mastering Control for Lasting Intimacy
Introduction to the Squeeze Technique The Squeeze Technique, sometimes referred to as the Masters and Johnson technique, is a highly regarded behavioral method developed within sex therapy for the management and treatment of premature ejaculation (PE). This technique is fundamentally based on the principle of gradually increasing the male partner’s tolerance for high levels of […]

Sexual Intimacy: The Psychology of Oral Pleasure
Definition and Terminology Fellatio is formally defined as the sexual act involving the use of the mouth, lips, tongue, and throat to provide tactile and sensory stimulation to the penis. This detailed definition encompasses a wide range of techniques and levels of intensity, focusing fundamentally on achieving sexual arousal or orgasm for the recipient. The […]

Autogenital Stimulation: Exploring Sexual Self-Discovery
Definition and Scope of Autogenital Stimulation Autogenital stimulation refers precisely to any deliberate action undertaken by an individual to stimulate his or her own genitalia for the express purpose of achieving sexual arousal, pleasure, or orgasm. This fundamental behavior is a core component of human sexuality and self-discovery, encompassing a wide spectrum of physical and […]
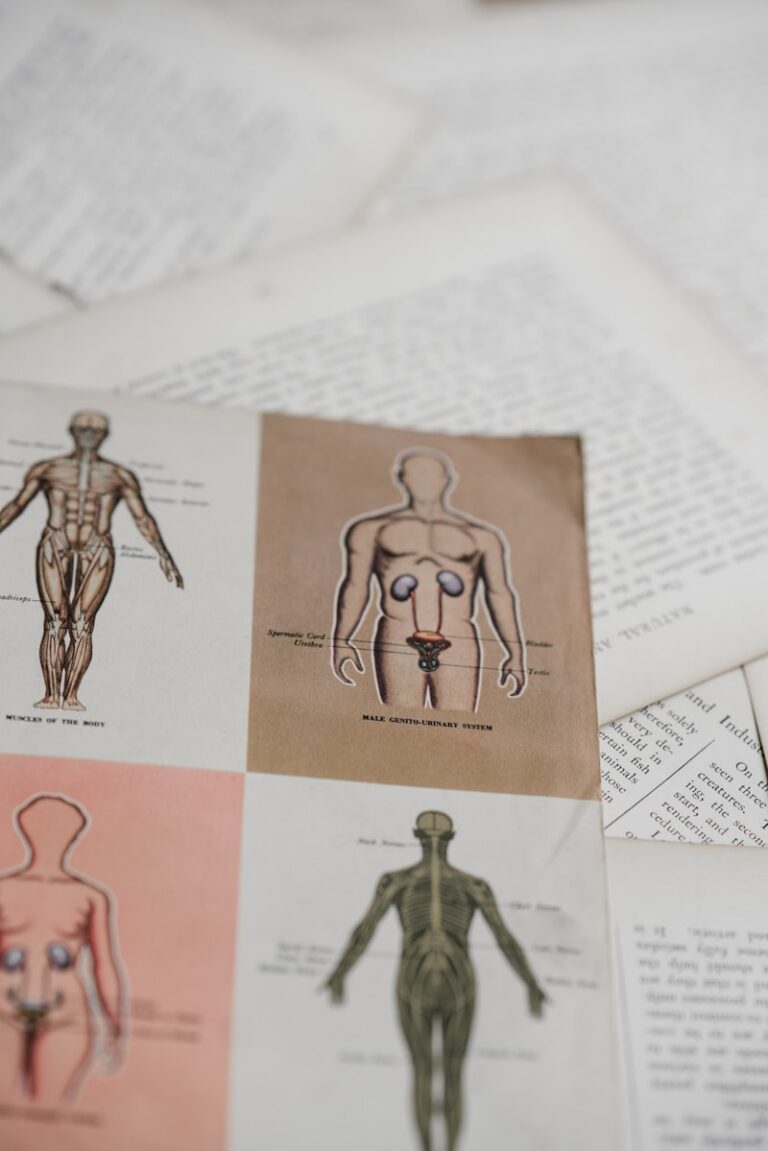
Sexual Anatomy: Beyond the Physical to Psychological Health
Introduction: Defining the Pudendum The term pudendum refers collectively to the female external sexual organs, serving as a comprehensive anatomical designation for the structures visible externally within the pelvic region. This area encompasses the entire superficial genital complex, acting as the external boundary that protects the delicate internal reproductive and urinary pathways. While technically a […]

Sexual Health Education: Empowering Knowledge for All
Introduction and Foundational Mission The Sexuality Information and Education Council of the United States, commonly known by its acronym SIECUS, stands as a pivotal non-profit organization dedicated to advocating for and promoting comprehensive sexuality education and accurate information about human sexuality across the nation. Established on the core belief that access to factual, age-appropriate, and […]
Psychogenic Vaginismus: Overcoming the Mind-Body Barrier
Introduction and Definition of Psychic Vaginismus Psychic vaginismus represents a severe manifestation of involuntary muscle spasms affecting the outer third of the vagina, specifically the pubococcygeus muscle complex. This condition is categorized fundamentally as a psychosexual disorder wherein psychological distress, fear, or anxiety triggers an extreme defensive physical reaction. It is characterized by an intense, […]
Spermatorrhea: Decoding the Psychology of Involuntary Loss
Definition and Clinical Description Spermatorrhea is clinically defined as the involuntary discharge of semen or seminal fluid without the presence of a preceding orgasm or sexual climax. Unlike nocturnal emissions, which are normal, physiological occurrences tied to sleep cycles and hormonal fluctuations, spermatorrhea is characterized by its sporadic nature and the absence of the typical […]
Anaphrodisiacs: Understanding the Science of Suppressed Libido
Definition and Etymology of Anaphrodisiacs The term anaphrodisiac refers to any narcotic, chemical agent, or substance that acts specifically to diminish or completely extinguish sexual desire, urges, and libido. Functionally, these agents serve as sexual relaxants or suppressants, operating in direct opposition to aphrodisiacs, which are intended to stimulate sexual appetite. While aphrodisiacs are often […]

Sociosexual Orientation: Decoding Your Intimacy Blueprint
Definition and Foundational Principles The Sociosexual Assessment constitutes a specialized psychological instrument designed to quantify an individual’s orientation toward sexual behavior, specifically focusing on the intersection between personal sexual activity and the prevailing cultural standards of commitment and relationship structure. This assessment meticulously measures a person’s intrinsic awareness of the established social norms regarding sexual […]

Parasexuality: Understanding Human Intimacy Beyond Norms
Definition and Conceptual Framework of Parasexuality The term parasexuality, while not officially recognized within the primary diagnostic manuals such as the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) or the International Classification of Diseases (ICD-11), functions in certain academic and clinical contexts as a descriptive umbrella for sexual actions that deviate significantly from established […]
Aphanisis: The Psychoanalytic Death of Desire
Introduction and Definition: The Core Concept Aphanisis is a term originating from early twentieth-century psychoanalytic theory, now considered largely obsolete within modern psychological and psychiatric nosology. The term was employed to denote the complete and total extinction of sexual desire, libido, or potency within an individual. Unlike conditions that might describe diminished or intermittent sexual […]

Sexual Negativism: Unlocking the Roots of Low Desire
Introduction and Definition of Sexual Negativism The concept of Sexual Negativism refers specifically to a profound and persistent reduction or complete absence of sexual interest and desire, a state which is centrally linked to measurable physiological deficits. Unlike other classifications of desire disorders that may stem primarily from psychological distress or relational conflict, the initial […]

Sexual Aversion Disorder: Understanding the Fear of Intimacy
Definition and Conceptualization of Sexual Aversion Disorder Sexual Aversion Disorder, historically recognized as a distinct clinical entity, is characterized by persistent or recurrent extreme aversion to, and active avoidance of, all or almost all genital sexual contact with a partner. This aversion is not merely a lack of interest or desire, but rather an intense, […]

Petting Behavior: Navigating Physical Intimacy in Teens
carnal activity which might not progress to orgasm or might be foreplay participated in before orgasm. Petting behavior might consist of kissing, oral sex, caressing the breasts and genitals and putting the genitals in apposition. PETTING BEHAVIOR: “Petting behavior is common in early adolescent relationships.”

Secondary Sexual Dysfunction: Restoring Your Intimate Flow
Introduction to Secondary Sexual Dysfunction Secondary Sexual Dysfunction (SSD) is defined as any disruption in typical sexual function that is acquired, meaning it manifests after a period of previously normal sexual functioning. Unlike primary sexual dysfunction, which characterizes lifelong difficulties experienced since the onset of sexual maturity, SSD is situational, temporary, or confined to specific […]

Male Sexual Identity: Beyond the Biological Basics
Introduction and Definition The penis is the primary external sexual and excretory organ in human males and other male mammals, serving essential dual functions within the body’s complex systems. Anatomically, it is a cylindrical structure designed for the conveyance of urine from the bladder, a process managed by the urinary tract, and crucially, for the […]
Sexuality Education: Empowering Healthy Human Development
Introduction and Definition of SIECUS The acronym SIECUS stands for the Sexuality Information and Education Council of the United States, a prominent national non-profit organization dedicated to affirming that sexuality is a natural and healthy part of human life and advocating for comprehensive sexuality education (CSE) for all individuals. Founded on the principle that accurate, […]

Sexual Contact: Understanding Intimacy and Human Connection
Definition and Scope of Sexual Contact Sexual contact is defined broadly within psychological and sociological frameworks as any form of physical interaction between individuals that involves overt or implied sexual intent, resulting in or aimed at achieving sexual arousal, gratification, or intimate bonding. This spectrum of behavior is extensive, encompassing interactions ranging from subtle, exploratory […]
Compulsive Sexual Behavior: Breaking the Cycle of Control
Defining Compulsive Sexual Behavior The concept of sexual addiction, or more formally referred to in certain diagnostic nomenclature as Compulsive Sexual Behavior Disorder (CSBD), describes a persistent and escalating pattern of sexual behavior characterized by a profound loss of control, intense preoccupation, and the continuation of these behaviors despite significant adverse consequences. This pattern closely […]
Autosexuality: Exploring the Psychology of Self-Arousal
Introduction and Definitional Framework Autosexuality, in the context of human sexuality and psychological study, refers broadly to any manifestation of sexual arousal or stimulation where the individual themselves is the sole source and object of the activity. This concept encompasses a range of behaviors and cognitive processes that yield sexual pleasure without requiring the physical […]
Sexual Dysfunction NOS: Understanding Residual Diagnoses
Definitional Context and Residual Classification The diagnostic category Sexual Dysfunctions Not Otherwise Specified (NOS) functions as a critical residual classification within clinical psychology and psychiatry. This designation is employed when an individual presents with significant sexual difficulties, distress, or impairment related to sexual functioning, but their specific presentation does not meet the full diagnostic criteria […]

SAR Workshops: Unmasking Biases to Transform Your Practice
Introduction to the Sexual Attitude Reassessment Workshop (SAR Workshop) The Sexual Attitude Reassessment Workshop, commonly abbreviated as the SAR Workshop, represents a highly specialized and intensive form of professional sex education. It is fundamentally a structured group experience designed not to impart specific sexual techniques or clinical skills, but rather to challenge and transform the […]
Sexological Assessment: Unlocking Sexual Well-being
Introduction and Definition of Sexological Examination The sexological examination constitutes a comprehensive, multidisciplinary assessment designed to systematically analyze and understand the determinants of an individual’s sexual behavior and function across the lifespan. This rigorous process moves beyond surface-level descriptions of conduct, aiming instead to delineate the complex interplay of factors that have shaped a person’s […]
Sexual Liberation: Breaking Free From Psychological Barriers
Introduction and Definitional Scope The concept of Sexual Liberation encompasses a complex interplay of individual agency and collective social reform, fundamentally defined by two interconnected processes. Firstly, it refers to the personal state of being free from restrictive sexual constraints, psychological inhibitions, and inherited moral judgments that traditionally limit healthy sexual expression. This deeply personal […]

Sexual Dysfunction: Navigating the Complexities of SDNOS
Introduction to Sexual Disorder Not Otherwise Specified (SDNOS) The designation Sexual Disorder Not Otherwise Specified (SDNOS) represents a crucial, yet often complex, diagnostic category within clinical psychology and psychiatry. It is utilized when a patient presents with a significant sexual problem that clearly requires clinical attention and causes measurable distress or impairment, but whose specific […]
Sexual Arousal: The Psychology Behind Your Desire
Definition and Neurobiological Foundations Sexual arousal is fundamentally defined as a complex physiological and psychological state triggered by exposure to sexual stimuli, which can manifest through direct physical contact, cognitive processes, or sensory input. This state represents the initial phase in the comprehensive sexual response cycle, acting as the critical bridge between neutral quiescence and […]
Sex-Positivity: Embracing Healthier Human Connections
Definition and Core Principles of Sex-Positivity The concept of sex-positivity represents a fundamental philosophical stance that views human sexuality, sexual activity, and sexual identities as inherently healthy, natural, and positive aspects of the human experience. Unlike traditional or conservative perspectives that often frame sex through the lens of danger, sin, or mandatory reproduction, sex-positivity asserts […]

Sexual Intimacy: The Psychology of Pleasure and Connection
Definition and Scope Cunnilingus is defined formally as the stimulation of the external female genitalia, primarily the clitoris, the clitoral hood, and the labia, using the tongue, mouth, or lips. This form of sexual expression is a common practice across many cultures globally, serving either as a dedicated act leading to orgasm or as a […]

Sexual Dysfunction: Understanding the Mind-Body Connection
Introduction and Definition of Sexual Dysfunction Sexual dysfunction is an umbrella term encompassing a heterogeneous group of conditions characterized by persistent or recurrent problems related to sexual response, desire, orgasm, or sexual pain, resulting in significant personal distress or interpersonal difficulty. These disorders fundamentally interfere with the individual’s ability to experience satisfaction during the various […]

Nocturnal Penile Tumescence: What Your Sleep Reveals
Nomenclature and Definition of Nocturnal Penile Tumescence The phenomenon commonly referred to as a morning erection is formally known within medical and sleep science literature as Nocturnal Penile Tumescence, or NPT. This physiological occurrence is characterized by the involuntary engorgement and subsequent complete erection of the penis, typically observed upon or shortly before waking. While […]

Self-Stimulation: Understanding the Psychology of Pleasure
is the process of manipulating ones own genital organs, whether a penis or clitoris for the purposes of self-stimulating removing the requirement for a partner. MASTURBATION: “Masturbation is the act of self-fulfilling an orgasm without the help of another, typically through observation of elicit material.”
The PLISSIT Model: A Guide to Addressing Sexual Wellness
Introduction to the PLISSIT Model The term PLISSIT is an acronym defining a widely recognized and utilized model for the assessment and management of patients presenting with sexual concerns or dysfunction. Developed by Dr. Jack S. Annon in the 1970s, this conceptual framework provides counselors, therapists, and healthcare professionals with a structured, tiered approach to […]

Sexual Health: The Psychology of Safer Intimacy
Definition and Historical Context The condom is defined fundamentally as a protective barrier device utilized during sexual intercourse, typically fabricated from resilient materials such as latex or synthetic alternatives. Its primary function involves placement over the erect male genitalia to establish a physical barrier that prevents the exchange of bodily fluids. This mechanism serves two […]

Euphemisms: The Psychology of Sexual Slang
Introduction and Definition of “Rubber” The term rubber, within the context of sexual health and psychology, functions as a highly prevalent and informal synonym for a condom, specifically a male sheath designed for contraceptive use and the prevention of sexually transmitted infections (STIs). This linguistic substitution is a classic example of metonymy, where the material […]
Human Sexuality: Beyond the Biology of Connection
Defining Sexuality: Beyond the Act Sexuality represents a profound and multifaceted element of the human condition, extending far beyond simple biological functions or reproductive drives. It is an intricate synthesis of biological mechanisms, psychological experiences, sociocultural influences, and ethical considerations. Fundamentally, sexuality encompasses the total expression of ourselves as sexual beings, including our thoughts, fantasies, […]

Male Orgasmic Disorder: Decoding the Delay in Pleasure
Definition and Classification of Male Orgasmic Disorder Male Orgasmic Disorder (MOD), often clinically referred to as Delayed Ejaculation (DE), is classified in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), as a sexual dysfunction characterized by a persistent or recurrent delay in, or absence of, male orgasm following adequate sexual stimulation and […]

Sexual Dysfunction: Understanding Retrograde Ejaculation
Definition and Fundamental Mechanism Retrograde ejaculation is a specialized form of male sexual dysfunction characterized by the seminal fluid, which is typically expelled forward through the urethra during orgasm, being rerouted backward into the urinary bladder. This physiological deviation occurs during the emission and expulsion phases of the ejaculatory process. Normally, the muscular sphincter located […]
Sexual Erethism: Understanding Persistent Genital Distress
Introduction and Definition of Sexual Erethism Sexual Erethism, historically recognized within psychosexual literature, describes a specific, distressing condition characterized by an abnormal irritability or an intensely unpleasant sensation centered in the sexual organs. This state is fundamentally distinct from typical sexual arousal, as the sensations experienced are perceived not as pleasurable or desirous, but as […]

Sexology: Unveiling the Science of Human Intimacy
Defining Sexology: Scope and Purpose Sexology is formally defined as the rigorous, multidisciplinary scientific study of human sexuality, encompassing all facets of sexual life. At its core, this discipline seeks to objectively understand and analyze the biological, psychological, sociological, and cultural dimensions that shape sexual identity, behavior, and interaction across the lifespan. Unlike casual observation […]
Anorgasmia: Overcoming Barriers to Sexual Fulfillment
Introduction and Definition Anorgasmia, derived from the Greek meaning “without swelling” or “without passion,” is formally defined in the clinical context as the persistent or recurrent difficulty, delay in, or total inability of an individual to achieve orgasm following sufficient sexual stimulation and arousal. This condition is categorized within the spectrum of sexual dysfunction disorders, […]

Detumescence: The Science of Physiological Recovery
Detumescence: The Physiological Mechanism of Subsiding Swelling The Core Definition of Detumescence Detumescence is defined formally as the process of lessening or subsiding of swelling, particularly referring to the reduction in size and rigidity of erectile tissue following a state of engorgement. This term is most frequently utilized within the context of human physiology, specifically […]
Atypical Psychosexual Dysfunction: Navigating Hidden Hurdles
Atypical Psychosexual Dysfunction Core Definition and Classification Atypical Psychosexual Dysfunction represents a category within clinical Psychiatry and clinical psychology reserved for sexual difficulties that defy precise categorization within established diagnostic schemata. Fundamentally, it is a sexual problem or concern that causes significant distress or interpersonal difficulty but fails to meet the specific diagnostic criteria for […]
Biological Drives: The Psychology of Seminal Influence
Semen (Seminal Fluid) The Core Definition and Composition Semen, often referred to synonymously as seminal fluid, is the complex, heterogeneous biological material expelled from the male reproductive tract during the process of ejaculation. Far from being a simple, monolithic fluid, semen represents a carefully calibrated cocktail of cellular components—primarily spermatozoa—suspended within a nutrient-rich and protective […]

Sexual Health: The Psychology of Intimate Well-Being
Sexual Hygiene The Foundation of Sexual Hygiene Sexual hygiene, often referred to simply as sex hygiene, encompasses the comprehensive set of practices and behaviors designed to maintain health, prevent the transmission of illness, and promote overall well-being related to sexual activity and the genital areas. It extends far beyond basic sanitation, integrating aspects of preventative […]

Spectatoring: Overcoming Performance Anxiety in the Bedroom
SPECTATOR ROLE: Performance Anxiety in Sexual Function The Core Definition of Spectatoring The concept known as the Spectator Role describes a specific pattern of cognitive and emotional behavior in which an individual’s natural sexual and physiological responses are significantly impaired or completely blocked due to intense, self-focused performance anxiety. At its core, this psychological state […]
Apareunia: Understanding Barriers to Intimacy
Apareunia 1. The Core Definition of Apareunia Apareunia is fundamentally defined as the inability or sustained refusal to engage in sexual intercourse, specifically referring to the absence of penile-vaginal penetration or coitus. This term encompasses two distinct, though often conflated, psychological and physiological states. In its primary clinical usage, apareunia denotes a physical or psychological […]

Fellatio: The Psychology of Intimate Oral Connection
Fellatio: Psychological and Sexual Health Perspectives Definition and Terminology The common colloquialism “blow job” is a widely recognized slang term referring to the sexual act of fellatio, which is defined formally as the oral stimulation of the penis. This act is performed by a partner using the mouth, tongue, lips, and throat. In the context […]

Human Sexuality: The Psychology Behind Ejaculation
Seminal Discharge: Definition, Mechanism, and Psychological Context The Core Definition and Fundamental Mechanism Seminal discharge, scientifically termed Ejaculation, refers to the reflex process involving the propulsion and ejection of semen from the male reproductive tract, typically through the urethra and out of the body. This complex physiological event is the culmination of the male sexual […]

Tantric Intimacy: Elevating Human Connection and Vitality
It is an approach that highly values sex and according to this Chinese based philosophical approach towards sex have the belief that immortality can be reached by doing regular sex. TANTRIC SEX: “Tantric Sex approach is in favour of sex to reach immortality.”
Musturbation: Breaking Free From Perfectionist Demands
Musturbation: The Core of Irrational Beliefs in REBT The Core Definition of Musturbation Musturbation is a term coined by the influential psychologist Albert Ellis, the founder of Rational Emotive Behavior Therapy (REBT). It serves as a memorable, slightly provocative shorthand for the absolute, demanding beliefs that Ellis identified as the primary source of human psychological […]

Sexual Burnout: Reclaiming Intimacy and Passion
Sexual Burnout The Core Definition of Sexual Burnout Sexual burnout is a specific psychological state characterized by chronic exhaustion and diminished motivation concerning sexual activity, often experienced within the context of a long-term relationship. It is crucial to distinguish sexual burnout from temporary periods of low libido or fatigue, as the former represents a pervasive […]
Sexual Anesthesia: When Desire Fades Into Silence
Sexual Anesthesia: A Psychological and Clinical Overview The Core Definition of Sexual Anesthesia Sexual Anesthesia, while not a formal diagnostic term in contemporary psychiatric manuals such as the DSM-5, refers clinically and conceptually to a profound, persistent state characterized by the absence or severe reduction of subjective sexual excitement, responsiveness, and desire. In essence, it […]
Erectile Dysfunction: Unmasking the Mind-Body Connection
Erectile Dysfunction: Etiology, Impact, and Treatment The Core Definition of Erectile Dysfunction Erectile dysfunction (ED), often referred to colloquially as impotence, is defined medically as the consistent or recurrent inability to attain or maintain a penile erection sufficient for satisfactory sexual performance. This condition is notably common, affecting a significant percentage of the adult male […]
Bondage: The Psychology of Power and Trust
Bondage: Psychological Dimensions and Ethical Practice The Core Definition and Scope of Bondage Bondage, in the context of human sexuality and relationship dynamics, is defined as a specific form of sexual expression involving the physical and psychological restriction of one partner by another, or sometimes, self-imposed restriction. At its foundation, Bondage is characterized by the […]

Anal Sexuality: Understanding Human Intimacy and Health
Anal Intercourse: Psychological, Health, and Social Perspectives The Core Definition and Mechanism Anal intercourse is broadly defined as a sexual activity involving the insertion of the penis, fingers, or objects into the anus and rectum. While historically and socially associated primarily with sexual activity between men, modern data collected by sexologists and public health researchers […]

Sexual Dysfunction: Understanding the Barriers to Intimacy
Sexual Disorders: An Encyclopedia Entry The Core Definition of Sexual Disorders A sexual disorder, often referred to synonymously in clinical settings as Sexual dysfunction, is broadly defined as a condition that prevents an individual or a couple from experiencing satisfaction or fulfillment during any phase of the sexual response cycle. This inability to enjoy or […]
Sexual Latency: Why Desire Sometimes Goes Silent
SEXUAL LATENCY The Core Definition of Sexual Latency Sexual latency, in a contemporary clinical context, is a term utilized to describe a significant and often distressing period marked by a decreased level of sexual activity or a pronounced lack of sexual desire (libido) in an individual who previously experienced a typical level of sexual interest. […]

Behavioral Sex Therapy: Reclaiming Intimacy Through Action
Behavioral Sex Therapy The Core Definition of Behavioral Sex Therapy Behavioral Sex Therapy (BST) is a specialized, goal-oriented form of psychotherapy designed specifically to treat issues related to sexual dysfunction and dissatisfaction. At its core, BST focuses not primarily on deep, unconscious conflicts, but rather on overt behaviors, cognitions, and emotional responses that interfere with […]

Sexual Orgasm: The Science of Peak Pleasure
The Psychology and Physiology of Orgasm The Core Definition of Orgasm The orgasm, derived from the Greek word meaning “to swell or become excited,” is defined as the climax of the human sexual response cycle. It is a highly pleasurable, transient peak sensation of intense physical and psychological release, typically experienced following adequate sexual stimulation. […]
Sexual Apathy: Understanding the Root of Low Desire
Sexual Apathy: An Encyclopedia Entry The Core Definition of Sexual Apathy Sexual apathy is fundamentally defined as a pervasive and persistent lack of interest in sexual activity, often encompassing a decreased or entirely absent desire for sex, coupled with difficulty achieving or maintaining sexual arousal. It differs significantly from a temporary dip in libido, instead […]
Celibacy: The Psychology of Voluntary Abstinence
Celibacy: A Psychological and Cultural Overview Defining Celibacy The term Celibacy is fundamentally defined as the state of voluntarily abstaining from sexual activity, sexual relations, or marriage, often maintained for a significant period or for life. While the most common understanding centers on the cessation of sexual intercourse, the concept often encompasses broader definitions depending […]

Sexual Sensation: The Science of Intimate Connection
The Psychology and Physiology of Sexual Sensation The Core Definition and Mechanism Sexual sensation, often colloquially referred to as “sex feeling,” is defined as the holistic constellation of emotional, cognitive, and physical responses experienced by an individual in the context of sexual activity. It is a profoundly complex and highly individualized experience that encompasses much […]

Sexual Intimacy: Enhancing Connection Through Shared Pleasure
Mutual Masturbation in Psychological and Relational Contexts Definition and Core Mechanisms Mutual masturbation is defined concisely as the shared act of providing or receiving manual, oral, or other non-penetrative stimulation of the genitals between two or more individuals, specifically for the purpose of achieving or enhancing sexual pleasure. This activity is a distinct form of […]
Testosterone: The Hidden Engine of Human Behavior
Testosterone: A Comprehensive Encyclopedia Entry The Core Definition of Testosterone Testosterone is a crucial steroid hormone belonging to the androgen group, primarily recognized for its pivotal role in male sexual development and reproductive function. However, its influence extends far beyond these primary functions, impacting a vast array of physiological processes in both men and women. […]

Sexual Response: Decoding Your Body and Mind
Sexual Response The Core Definition of Sexual Response The sexual response cycle is a complex and dynamic physiological and psychological process that describes the sequence of changes individuals experience during sexual activity. Fundamentally, it encompasses a series of bodily and mental transformations, originating from various forms of stimulation, ultimately leading to orgasm and subsequent resolution. […]
Sexual Inhibition: Unlocking Your Hidden Desire
Sexual Inhibition The Core Definition of Sexual Inhibition Sexual inhibition is a profound psychological concept characterized by a reluctance, aversion, or unwillingness to engage in sexual activities or to express oneself sexually. This multifaceted phenomenon extends beyond simple disinterest, encompassing a spectrum of internal and external factors that suppress or impede a healthy and fulfilling […]
Sexual Adjustment: Finding Harmony in Intimacy
Sexual Adjustment The Core Definition of Sexual Adjustment Sexual adjustment is a multifaceted and dynamic concept within the field of psychology that encompasses the harmonious integration of an individual’s physical, psychological, and social dimensions concerning their sexual functioning and overall satisfaction. It extends beyond the mere absence of sexual dysfunction, delving into the subjective experience […]

Sexual Counseling: Reclaim Your Intimacy and Connection
SEXUAL COUNSELING The Core Definition Sexual counseling is a specialized form of psychotherapy meticulously designed to assist individuals, couples, or families in comprehensively addressing and effectively resolving a broad spectrum of issues pertinent to sexual behavior and sexuality. It extends beyond mere problem resolution, encompassing crucial areas such as the identification and adept management of […]

Androgen: How Hormones Shape Your Behavior and Mind
Androgen Core Definition of Androgens Androgens represent a crucial class of hormones, primarily recognized for their pivotal role in regulating the development and maintenance of male sexual characteristics and reproductive functions. These powerful steroid hormones are instrumental in orchestrating a wide array of biological processes that extend far beyond sexual differentiation, influencing metabolism, bone health, […]