
Delayed Response: Mastering the Art of Intentional Action
DELAYED RESPONSE Introduction to Delayed Response The concept of delayed response (DR) describes a fundamental psychological phenomenon where an organism’s reaction to a specific stimulus or event is not immediate but occurs after a measurable period of time has elapsed. This delay is not merely a passive waiting period; rather, it often involves active cognitive […]
Delta Waves: The Secret Science of Deep Restorative Sleep
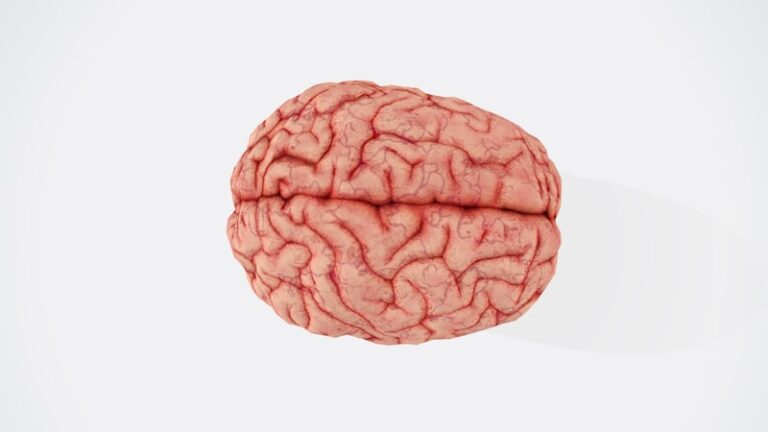
Delta Waves Core Definition of Delta Waves Delta waves are a distinct type of high-amplitude, low-frequency brain wave predominantly associated with the deepest stages of sleep, specifically non-rapid eye movement (NREM) sleep stage N3, which was formerly known as stages 3 and 4. These powerful brain oscillations are characterized by their slow frequency range, typically […]

Degrees of Freedom: Unlocking Your Cognitive Potential
Degrees of Freedom The Core Definition of Degrees of Freedom The concept of degrees of freedom (often abbreviated as DOF) is a fundamental analytical tool employed across various scientific and engineering disciplines, including its crucial applications within psychology. At its most basic, DOF quantifies the number of independent variables that must be known to precisely […]
Déjà Raconte: The Psychology of Retold Memories
DEJA RACONTE: A Comprehensive Encyclopedia Entry The Core Definition of Deja Raconte Deja Raconte is an innovative digital storytelling platform designed to empower users to create and share interactive narratives through a user-friendly web-based application. At its heart, it provides a robust toolkit for transforming traditional narratives into dynamic, engaging experiences that can be shared […]
Deferred Imitation: How Children Learn from Memory
Deferred Imitation The Core Definition of Deferred Imitation Deferred imitation is a fascinating phenomenon in developmental psychology where an individual observes an action performed by another person and then reproduces that action at a later time, when the original model is no longer present. This ability signifies a crucial step in cognitive development, moving beyond […]

Defect Orientation: Overcoming the Bias of Imperfection
Defect Orientation (Psychology) The Core Definition In the realm of psychology, Defect Orientation refers to a distinct cognitive and perceptual bias where an individual consistently and often disproportionately focuses on perceived flaws, imperfections, or negative attributes—referred to as “defects”—in themselves, others, or various situations. This mental filter tends to magnify deficiencies while often diminishing or […]

Psychological Disorder: Decoding the Chaos of the Mind
Disorder The Core Definition of Disorder The concept of disorder fundamentally refers to a state characterized by a lack of order, structure, or typical functioning, often leading to confusion, disruption, or deviation from expected norms. While broadly applicable across various domains, from physical systems to societal structures, in psychology, the term primarily denotes a significant […]
Disengagement Theory: The Psychology of Social Withdrawal
Disengagement Theory: An Encyclopedia Entry Core Definition of Disengagement Theory Disengagement theory is a foundational concept in the field of gerontology and developmental psychology, proposing that as individuals enter later life, a mutual process of withdrawal or separation occurs between them and society. This theory suggests that it is a natural, inevitable, and often functional […]

Discrete Data: Counting the Building Blocks of Human Behavior
Discrete Data The Core Definition of Discrete Data Discrete data constitutes a fundamental type of data characterized by its distinct, separate, and countable values. Unlike data that can theoretically assume any value within a given range, discrete data is constrained to a finite or countably infinite set of specific, isolated points. Each value stands alone, […]

Discrimination Reaction Time: How Fast Do You Process?
Discrimination Reaction Time Introduction: Defining Discrimination Reaction Time Discrimination Reaction Time (DRT) is a sophisticated metric within the domain of cognitive psychology, specifically designed to quantify the speed and efficiency with which an individual can process multiple sensory inputs, distinguish a particular target stimulus from distractors, and subsequently initiate an appropriate motor response. It stands […]
Discomfort Anxiety: Why You Avoid Feeling Unwell
Discomfort Anxiety: A Comprehensive Encyclopedia Entry The Core Definition of Discomfort Anxiety Discomfort anxiety is a specific type of anxiety characterized by significant emotional distress and avoidance behaviors in response to situations or sensations of physical or psychological discomfort. It goes beyond a typical aversion to unpleasant experiences; instead, individuals with discomfort anxiety experience profound […]
Epigenetic Memory: How Chromatin Shapes Your Mind
DIRHINIC: Differential Impact of Regulatory Histone Modifications Associated with Chromatin Interactions The Core Definition of DIRHINIC The term DIRHINIC, an acronym for Differential Impact of Regulatory Histone Modifications Associated with Chromatin Interactions, refers to an innovative and sophisticated method developed for the comprehensive detection of multiple types of epigenetic modifications. This technique addresses a longstanding […]

Dipsomania: Understanding the Cycle of Compulsive Drinking
Dipsomania: A Comprehensive Encyclopedia Entry The Core Definition Dipsomania is a historical term used to describe an intense, uncontrollable, and often periodic craving for alcoholic beverages, leading to episodes of compulsive consumption. It represents a profound inability to resist the urge to drink, often culminating in severe intoxication. While the term itself has largely been […]
Directed Reverie: Unlock Your Mind Through Guided Imagery
Directed Reverie: A Therapeutic Approach Introduction to Directed Reverie Directed Reverie is an innovative and increasingly recognized therapeutic approach within the field of mental health, characterized by its utilization of guided imaginative experiences. At its core, this therapy facilitates a structured journey into an individual’s inner world, employing a series of carefully constructed mental images […]
Dihydrocodeine: The Psychology of Pain and Opioid Relief
Dihydrocodeine: A Comprehensive Encyclopedia Entry Core Definition and Mechanism Dihydrocodeine (DHC) is a semi-synthetic opioid analgesic medication primarily utilized for the relief of moderate to severe pain. It is classified as an opiate, a class of drugs derived from the naturally occurring alkaloids found in the opium poppy plant. Specifically, DHC is synthesized from codeine, […]

Biological Dimorphism: Why Opposites Attract and Differ
Dimorphism The Core Definition of Dimorphism Within the vast diversity of the biological world, dimorphism stands as a compelling phenomenon where two distinct forms of individuals exist within the same species. These forms are characterized by observable differences in morphology, physiology, or behavior, which are not merely individual variations but represent consistent, alternative expressions within […]
Diffuse Thalamic Projection System: The Brain’s Gateway
Diffuse Thalamic Projection System (DTPS) The Core Definition of the Diffuse Thalamic Projection System The Diffuse Thalamic Projection System (DTPS) represents the most extensive network of projections originating from the thalamus within the central nervous system, distributing its intricate neuronal connections across virtually the entire neocortex. This complex system is characterized by a vast multitude […]
Differential Fertility: Why Reproductive Rates Vary
DIFFERENTIAL FERTILITY Introduction to Differential Fertility Differential fertility refers to the phenomenon where different population subgroups exhibit varying levels of fertility rates. This core concept is fundamental to understanding the dynamics of population growth, composition, and change over time. It posits that reproductive patterns are not uniform across an entire society but are systematically influenced […]

Dietary Selection: The Psychology of What We Choose
Dietary Selection The Core Definition of Dietary Selection Dietary selection refers to the intricate process by which humans and animals choose what to consume from the vast array of available food options. This fundamental biological and behavioral phenomenon is not merely a simple act of eating but a complex interplay of internal and external factors […]
The Dice Model: Mastering Complex Human Systems
The Dice Model: A Framework for Understanding Complex Systems The Core Definition of the Dice Model The Dice Model, also recognized as the Dice-Luhmann model, represents a theoretical framework designed for the description and prediction of behavior within complex systems. At its essence, the model posits that any intricate system, irrespective of its domain—be it […]
Sociolinguistics: Decoding How Our Speech Shapes Identity
Dialectology Introduction to Dialectology: The Study of Language Variation Dialectology represents a specialized branch within the broader discipline of linguistics, primarily concerned with the systematic investigation of dialects and language varieties. It delves into the intricate patterns of linguistic diversity, seeking to understand how language manifests differently across geographical regions, social groups, and even among […]
Chirality: How Molecular Direction Shapes Our Mental State
Dextro- (DEXTR-) Dextrorotation and Optical Activity: The Core Definition The term dextro- (or dextr-) originates from the Latin word “dexter,” meaning “right,” and is fundamentally used in chemistry to describe substances that exhibit a specific interaction with polarized light. More precisely, a dextro- compound is characterized by its ability to rotate the plane of plane-polarized […]

Diagnostic Classification: Mapping Patient Care Outcomes
Diagnosis-Related Groups (DRGs) The Core Definition of Diagnosis-Related Groups (DRGs) Diagnosis-Related Groups (DRGs) represent a pivotal system within health care reimbursement, primarily utilized in the United States and adopted by numerous other nations. At its fundamental level, a DRG serves as a patient classification scheme that categorizes hospital inpatient services into groups of clinically coherent […]

Developmental Systems: Unlocking Lifespan Growth Potential
Developmental Systems Approach Understanding the Developmental Systems Approach: The Core Definition The Developmental Systems Approach (DSA) represents a comprehensive and highly influential theoretical framework within the field of psychology and related disciplines, offering a sophisticated lens through which to understand the intricate processes of development across the lifespan. At its core, DSA posits that individual […]
Psychological Deterrence: Mastering the Art of Influence
Deterrence in International Relations and Psychology The Core Definition of Deterrence Deterrence, at its most fundamental level, is a psychological strategy aimed at preventing an undesirable action by instilling fear of the consequences. It operates on the principle that a rational actor, when confronted with the credible threat of unacceptable costs or punishment, will choose […]
Developmental Assessment: Mapping Your Child’s Growth
Developmental Assessment Core Definition of Developmental Assessment Developmental assessment is fundamentally a comprehensive, multi-disciplinary process designed to systematically gather and interpret detailed information about a child’s developmental trajectory. It serves as a critical diagnostic tool, moving beyond simple screening to provide an in-depth understanding of a child’s progress across various domains from birth through adolescence. […]
Design Trade-offs: The Psychology of Perfect Choices
Design Trade-off The Core Definition of Design Trade-off A design trade-off is a fundamental concept in engineering design and product design, referring to the necessary act of compromising or balancing competing objectives during the development process. In essence, it acknowledges that achieving all desirable attributes to their maximum potential simultaneously is often impossible due to […]
Detached Personality: The Psychology of Emotional Distance
Detached Character: An Encyclopedia Entry Introduction to Detached Character The concept of detached character represents a significant area of inquiry within psychological research, referring to a discernible pattern of interpersonal avoidance and a marked indifference to the emotional states of others. This disposition extends beyond mere introversion, delving into deeper aspects of emotional disengagement and […]

Dereism: Unlocking the Hidden Patterns of Human Thought
Dereism: A Unifying Paradigm for Human Cognition Introduction to Dereism Dereism represents a novel and ambitious framework within the study of cognition, positing itself as a unifying paradigm for understanding the intricate mechanisms of the human mind. At its core, Dereism proposes that the complex properties of cognition are not irreducible wholes but rather emergent […]
Decreolization: When Languages Lose Their Unique Identity
Decreolization: A Comprehensive Encyclopedia Entry Introduction to Decreolization Decreolization is a fascinating and intricate linguistic phenomenon describing the process by which a creole language gradually loses its unique structural and lexical characteristics, converging towards a more established and often socially dominant standard language. This transformation typically involves the assimilation of features such as a more […]
Descending Tracts: The Neural Pathways of Human Action
Descending Tracts Introduction to Descending Tracts The intricate orchestration of movement, posture, and vital internal functions within the human body relies fundamentally on a complex network of neural pathways. Among these, the descending tracts represent a critical component, serving as the primary communication channels through which the brain transmits commands and regulatory signals to the […]
The Deep-Pockets Effect: Wealth Disparity and Your Health
The Deep-Pockets Effect: Understanding Wealth Inequality and Health Outcomes Introduction to the Deep-Pockets Effect The Deep-Pockets Effect, a concept gaining increasing recognition in public health and social sciences, describes the distinct and often divergent health outcomes observed between individuals of differing wealth levels. It posits that a significant disparity in economic resources directly contributes to […]

Decision-Making Models: Empowering Your Client Choices
The decision-making model of counseling is a theoretical framework for understanding the process of counseling. It is based on the notion that individuals in counseling have decision-making abilities and that counselors should use this knowledge to assist their clients in making informed decisions. This model has been applied in various contexts, such as psychotherapy, career […]
Dyspnea: The Hidden Psychological Toll of Breathlessness
Dyspnea The Core Definition of Dyspnea Dyspnea, commonly known as shortness of breath, is a profoundly distressing and subjective experience characterized by an uncomfortable awareness of difficult or labored breathing. It is not merely a physical sensation but a complex perceptual phenomenon that can significantly impair an individual’s quality of life. This feeling of inadequate […]
Muscular Dystrophy: The Psychology of Resilience and Mind
Dystrophy: An Encyclopedia Entry Understanding Dystrophy: A Core Definition Dystrophy is an overarching term encompassing a group of diverse genetic disorders that are primarily characterized by the progressive deterioration and weakness of skeletal muscles. This debilitating condition arises from defects in the genes responsible for producing proteins essential for healthy muscle function. When these vital […]
Dysorexia: When Your Senses Mislead Your Mind
Dysorexia Introduction to Dysorexia Dysorexia is posited as a complex neurological disorder that fundamentally impacts an individual’s capacity to accurately process and comprehend sensory information received from their environment. This condition is characterized by significant difficulties in interpreting and appropriately responding to various external stimuli, encompassing a broad spectrum of sensory inputs such as sound, […]
Dynamogenesis: How Physical Movement Shapes Your Mind
Dynamogenesis: The Physiological Basis and Psychological Significance of Muscle Contractions The Core Concept of Dynamogenesis Dynamogenesis, in a physiological context, refers to the fundamental process of muscle contractions that are absolutely essential for a vast array of physiological functions within the human body. This intricate biological mechanism underpins everything from the most subtle movements of […]

Sleep Disorders: Unlocking the Mystery of Restful Nights
Sleep is essential for physical and mental health; however, disturbances in sleep can have serious consequences. Dysfunctions associated with sleep, sleep stages, or partial arousal are common among individuals of all ages and can have adverse health effects. These dysfunctions can range from difficulty falling asleep and staying asleep to increased risk of developing other […]
Dusky Standard: Mastering the Psychology of Thermal Comfort
The Dusky Standard (DS) The Core Definition of the Dusky Standard The Dusky Standard (DS) represents a novel and sophisticated quantitative framework designed for the comprehensive evaluation of thermal comfort in human occupants across a diverse range of indoor and outdoor environments. At its heart, the DS provides a refined metric that moves beyond traditional […]

Dynamic Core: Aligning Body and Mind for Peak Stability
Dynamic Core: An Integrated Approach to Physical and Psychological Well-being Core Definition and Foundational Principles The concept of Dynamic Core, as initially developed by physical therapist and strength and conditioning specialist Mike Robertson, represents a comprehensive fitness program meticulously engineered to enhance the strength, stability, and power of the body’s central musculature. It is fundamentally […]
Dual Attitudes: Why Your Gut and Brain Disagree
Dual Attitudes: Understanding the Interplay of Thought and Emotion in Behavior The Core Definition of Dual Attitudes Attitudes represent fundamental evaluations of people, objects, ideas, or activities that serve as the bedrock for how individuals perceive and engage with their surrounding environment. These deeply ingrained predispositions function as crucial mental shortcuts, enabling us to efficiently […]
Dual-Task Performance: Mastering the Art of Multitasking
Dual-Task Performance The Core Definition Dual-task performance is a fundamental concept within cognitive psychology that refers to an individual’s capacity to execute two distinct cognitive tasks simultaneously. At its essence, this paradigm serves as a critical cognitive assessment tool, designed to meticulously evaluate the human brain’s ability to allocate attentional resources and process information when […]
Droperidol: Neuroleptic Mechanisms and Clinical Efficacy
Droperidol: An Overview of its Pharmacology and Clinical Applications Introduction to Droperidol Droperidol, identified by its International Nonproprietary Name (INN) and known by the trade name Droleptan, represents a significant compound within the field of modern pharmacology. It is categorized as an antipsychotic drug, specifically belonging to the butyrophenone class. This classification immediately signals its […]

DREAMY STATE
Dreamy State: A Comprehensive Encyclopedia Entry Introduction to Dreamy States The concept of “dreamy states” represents a fascinating intersection of neurology and psychology, offering a unique lens through which to understand human consciousness and its various manifestations. These states are not merely about sleep-induced dreams but refer to a waking or semi-waking experience characterized by […]
Dramatization: Unleashing Empathy Through Role-Play
Dramatization: A Powerful Tool in Education Introduction to Dramatization Dramatization, in an educational context, refers to a pedagogical approach that leverages theatrical techniques and role-playing to actively engage students in the learning process. It transcends mere performance, serving as a dynamic method through which learners can explore, embody, and interpret academic content, personal experiences, and […]
Pathological Doubt: Breaking Free from Endless Uncertainty
Doubting Mania: A Comprehensive Psychological Overview The Core Definition of Doubting Mania Doubting mania, while not a formal diagnostic term in contemporary psychiatric manuals, serves as a vivid historical and descriptive label for a profound psychological state characterized by an intense, pervasive preoccupation with doubt and uncertainty. Individuals experiencing what has been colloquially termed “doubting […]
Dual-Process Theory: How Your Brain Makes Decisions
Dual-Process Theory Introduction to Dual-Process Theory The concept of Dual-Process Theory stands as a foundational framework within modern psychology, offering a compelling explanation for the intricate mechanisms underlying human thought, judgment, and decision-making. This theoretical perspective posits that human cognition is not a monolithic operation but rather the product of two distinct, interacting systems or […]

Perceptual Shift: How Motion Colors Your Reality
The Doppler Effect Understanding the Core Principle The Doppler Effect describes a fundamental phenomenon in physics where the observed frequency or wavelength of a wave changes due to the relative motion between the wave source and the observer. This effect is not a change in the wave’s actual emitted frequency but rather an apparent shift […]

Mental Chronometry: Measuring the Speed of Thought
Donders’s Method Introduction to Donders’s Method Donders’s Method, often referred to as the “timing method” or mental chronometry, is a pioneering technique in psychology and physiology designed to quantify the duration of specific mental operations. Developed by the Dutch physiologist and psychologist Franciscus Cornelis Donders in the mid-19th century, this method involves systematically varying the […]

Home-Based Support: Empowering Independence at Home
Domiciliary Care Core Definition of Domiciliary Care Domiciliary care, often referred to interchangeably as home care, represents the provision of professional services and support designed to assist individuals in their own homes, enabling them to maintain independence, comfort, and a familiar environment. This form of care encompasses a broad spectrum of services tailored to meet […]
Doerfler-Stewart Test: Unmasking Organic vs. Psychogenic
Doerfler-Stewart Test Introduction to the Doerfler-Stewart Test The Doerfler-Stewart Test is a significant and widely adopted diagnostic framework in clinical psychology and medicine, specifically designed to aid clinicians in differentiating between psychogenic and organic causes of a patient’s presenting symptoms. In essence, it provides a structured approach to unravel the complex interplay between physical ailments […]
Diversity Training: Bridging Minds for Better Inclusion
Diversity Training Introduction to Diversity Training In an increasingly globalized and interconnected world, the fabric of organizations, communities, and societies is woven with diverse threads of backgrounds, experiences, and perspectives. This inherent variety, while a source of immense strength and innovation, can also present challenges related to understanding, communication, and unconscious biases. To navigate these […]

Distributive Justice: Why Fairness Matters in Society
Distributive Justice Core Definition Distributive justice is a fundamental concept concerned with the fair and equitable allocation of resources, benefits, and burdens among individuals or groups within a society. At its core, it addresses how societal goods—such as wealth, income, opportunities, and social status—and societal bads—like taxes and obligations—should be distributed to ensure fairness and […]

Dissociative Trance: Unlocking the Mystery of Altered States
Dissociative Trance Disorder The Core Definition of Dissociative Trance Disorder Dissociative Trance Disorder (DTD) is a psychological condition characterized by episodes of an altered state of consciousness, often referred to as a trance. These trance-like states involve a temporary and profound loss of the sense of personal identity or full awareness of one’s immediate surroundings. […]
Visual Perception: How Distorted Imagery Reveals Your Mind
Distorting-Video Procedure Introduction to the Distorting-Video Procedure in Psychology The Distorting-Video Procedure, within the realm of psychological research, refers to a systematic methodological approach involving the deliberate and controlled alteration of video stimuli to investigate various aspects of human cognition, perception, and emotion. Unlike its common technical definition in digital media production, where video distortion […]
Disruptive Behavior: Decoding Patterns for Better Outcomes
Disruptive behavior is a form of problem behavior that can have a negative impact on the functioning of a group, organization, or individual. It is characterized by behaviors that are rude, inappropriate, and uncooperative, and can impede the progress of a group or organization. This article will review the literature on the causes, effects, and […]
Discriminant Analysis: Predicting Human Behavior
Discriminant Analysis: A Comprehensive Overview The Core Definition of Discriminant Analysis Discriminant analysis is a fundamental statistical classification technique used to categorize observations into two or more predefined groups or classes. It achieves this by constructing a linear combination of predictor variables, known as a discriminant function, which maximizes the separation between these groups. This […]
Disease Trajectory: Mapping the Path of Mental Recovery
Disease Course The Core Definition of Disease Course The concept of disease course fundamentally refers to the trajectory and evolution of a disease or medical condition over a period of time, from its inception through its various stages of progression, remission, or resolution. It encapsulates the dynamic interplay of biological, psychological, and social factors that […]

Disorganized Offender: The Psychology of Impulsive Crime
Disorganized Offender Core Definition of the Disorganized Offender The disorganized offender represents a distinct classification within criminal psychology, characterized primarily by a profound lack of planning, organization, and sophistication in the commission of criminal acts. This individual typically operates on an impulsive basis, driven by immediate urges or emotional states rather than premeditated strategy. Unlike […]
Psychological Disintegration: When the Self Falls Apart
Psychological Disintegration The Core Definition of Psychological Disintegration Psychological disintegration refers to a profound and often distressing breakdown in the coherent organization of an individual’s mental processes, sense of self, or personality. This complex phenomenon manifests as a fragmentation of thought, emotion, perception, memory, and identity, leading to a loss of psychological unity and integrity. […]
Psychic Discharge: Mastering Emotional Release for Balance
Psychic Discharge Introduction to Psychic Discharge In the realm of psychology, particularly within psychoanalytic theory, the concept of psychic discharge refers to the process by which an individual releases pent-up mental or emotional energy, thereby reducing internal tension and restoring a state of equilibrium. This fundamental mechanism is central to understanding how the mind manages […]
Discourse Routines: Mastering the Art of Classroom Dialogue
Discourse Routine: A Tool for Enhancing Communication in the Classroom The discourse routine is an effective tool for improving communication in the classroom. This simple and consistent structure provides a useful framework for teachers and students to follow during classroom discussions. By providing a clear structure and expectations for communication, the discourse routine can enhance […]

Directed Thinking: Mastering Your Cognitive Focus
Directed Thinking Core Definition Directed thinking is a sophisticated cognitive process characterized by the intentional and systematic application of both analytical and creative strategies toward a specific goal, most often problem-solving or decision-making. It stands in contrast to more diffuse or associative forms of thought, emphasizing a deliberate and focused mental effort to navigate complex […]
Diminished Responsibility: When Mental Health Alters Justice
Diminished Responsibility Introduction to Diminished Responsibility Diminished responsibility is a significant legal concept, widely recognized as an affirmative defense in many common law jurisdictions, including parts of the United States, the United Kingdom, and Canada. At its core, this defense posits that a defendant’s mental capacity was substantially impaired at the time of committing a […]
Direct Aggression: Understanding the Roots of Conflict
Direct aggression is a type of behavior that is characterized by physical or verbal contact intended to cause harm to another person (Baron & Richardson, 1994). It is considered a form of interpersonal violence and is a major public health problem (World Health Organization, 2002). Direct aggression is associated with a number of adverse outcomes, […]

Cognitive Reframing: Master Your Mindset for Success
Diffraction Grating: A Comprehensive Overview Introduction Diffraction gratings are an important component of modern optics since they are used to analyze light spectra and diffract beams of light. These gratings are made up of a series of parallel, evenly spaced, and regularly spaced lines, which produce a wide range of diffraction angles and light intensities. […]
Diglossia: The Hidden Psychology of How We Speak
Diglossia is a term used to describe language situations in which two varieties of the same language, typically a high-prestige variety and a low-prestige variety, coexist in a given speech community (Gumperz & Wilson, 1971). The high-prestige variety, often referred to as the “H” variety, is typically used in formal situations, while the low-prestige variety, […]
Differential Emotions Theory: Decoding Your Hidden Feelings
Differential Emotions Theory (DET) is an influential theory in psychology developed by Carroll E. Izard in the early 1970s. DET posits that emotions are universal, distinct, and discrete, and that they can be studied and identified through facial expressions and behaviors. According to the theory, these emotions can be organized into four distinct classes, which […]
Diestrus: The Biology of Rest and Biological Readiness
Introduction Diestrus is the fourth and final stage of the four-stage estrous cycle in female mammals. During diestrus, the female’s body is preparing for either conception or the start of a new cycle. This stage is characterized by the absence of ovarian activity and the presence of high levels of progesterone. Understanding diestrus is essential […]
Dibenzothiazepine: Neurochemical Keys to Cognitive Health
Introduction Dibenzothiazepine (DBT) is a class of heterocyclic compounds that have been used in a variety of applications for decades. As a member of the dibenzothiazepine family, it is a known inhibitor of the enzyme cytochrome P450 (CYP) enzymes. DBT has been studied for its potential therapeutic applications, such as the treatment of cancer, inflammation, […]

Dialectical Operations: Bridging Minds and Digital Tools
Dialectical Operations Introduction to Dialectical Operations Dialectical Operations represent a contemporary and evolving approach within the field of Human-Computer Interaction (HCI), fundamentally transforming how users engage with digital systems. At its core, this paradigm redefines the interaction model from a series of discrete commands or selections into a fluid, interactive dialogue between the human and […]

Diadochokinesis: Mastering the Rhythm of Your Mind
Diadochokinesis Core Definition of Diadochokinesis Diadochokinesis is a specialized motor skill that encompasses the capacity to execute rapid, alternating movements with exceptional coordination and rhythmic precision. It represents a fundamental aspect of motor control, requiring the seamless and swift transition between two distinct, opposing actions. This ability is not merely about speed but also about […]
Motor Dexterity: Assessing Your Brain-Hand Connection
Dexterity Tests: A Comprehensive Encyclopedia Entry Introduction to Dexterity Tests Dexterity tests are a specialized category of psychometric tests designed to systematically evaluate an individual’s ability to perform precise physical tasks using their hands, fingers, and arms. These assessments delve into the intricate coordination between sensory input and motor output, providing a quantifiable measure of […]

Developmental Age: Beyond Birthdays to True Potential
Developmental Age (DA) Introduction to Developmental Age (DA) Developmental Age (DA) is a sophisticated measure used to quantify a child’s overall developmental level in comparison to their chronological age. Unlike simply counting years or months, DA assesses a broad spectrum of a child’s capabilities across multiple domains, including cognitive development, language acquisition, motor skills, social-emotional […]

Developmental Sequence: Mapping the Path to Human Growth
DEVELOPMENTAL SEQUENCE Understanding the Developmental Sequence: A Foundational Concept The developmental sequence, often referred to as developmental order or trajectory, represents the intricate and systematic process of change and continuity experienced by human beings from the moment of conception through to the culmination of adulthood. It encompasses a vast array of transformations across multiple domains, […]
Determinism: Are You Actually In Control?
Determinism in Psychology The Core Definition of Determinism Determinism is a fundamental philosophical and scientific belief asserting that all events, including human cognition, decision-making, and behavior, are entirely determined by antecedent causes and natural laws. This principle posits that every event is the inevitable outcome of prior states and events, forming an unbroken chain of […]
Desymbolization: Unveiling the Hidden Meaning of Thought
Desymbolization: Concepts and Applications in Text Processing The Core Definition of Desymbolization Desymbolization, within the domain of computational linguistics and text processing, is the systematic procedure of removing non-essential or extraneous symbolic representations from a given text. Fundamentally, it involves stripping away superficial layers to unveil the core informational content, rendering the text more suitable […]
Averaging Bias: Why Designing for Everyone Fails Anyone
Design for the Average Introduction to Design for the Average The concept of Design for the Average refers to an approach in product and system development where the primary focus is on meeting the needs and capabilities of the statistically “average” user. This methodological orientation often involves gathering data on a broad population, identifying central […]
Descending Pathways: How Your Brain Orchestrates Movement
Descending Pathway The Core Definition: Orchestrating Movement The Descending Pathway represents a fundamental and indispensable component of the central nervous system, specifically critical to the neural circuits responsible for regulating voluntary and involuntary movement. At its essence, it constitutes a complex network of neurons originating in various regions of the brainstem and extending caudally into […]

Derealization: Navigating the World Through a Fog
Derealization: An Encyclopedia Entry Introduction to Derealization Derealization is a complex and often distressing dissociative experience characterized by a profound feeling of detachment from one’s surroundings. Individuals experiencing derealization perceive the external world as unreal, dreamlike, foggy, distant, or distorted. This sense of unreality extends to the environment, objects, and even other people, who may […]
Deprivation Index: Mapping Hidden Socio-Economic Stress
Deprivation Index The Core Definition of the Deprivation Index The Deprivation Index (DI) is a sophisticated composite measure designed to quantify and assess socio-economic disadvantage across various contexts, including communities, households, and individuals. At its most fundamental level, it serves as a crucial tool for understanding and mapping the living conditions that contribute to social […]
Depletive Treatment: Clearing Mental Blocks for Clarity
Depletive Treatment: A Comprehensive Overview The Core Definition of Depletive Treatment Depletive treatment represents a distinctive approach within healthcare, characterized by its multi-modal strategy aimed at alleviating symptoms associated with a diverse range of illnesses. At its core, this treatment modality integrates pharmaceutical interventions, precise dietary adjustments, and comprehensive lifestyle modifications. The fundamental premise is […]
Cognitive Doubt: Why Your Uncertainty is a Hidden Strength
Doubt: Its Role in Psychology and Society The Core Definition of Doubt At its fundamental level, doubt is defined as a feeling of uncertainty or a lack of conviction concerning the truth, reality, or reliability of something. This cognitive and emotional state involves a suspension of judgment or belief, often arising when an individual is […]
Psychomotor Assessment: Precision Testing for Brain Health
The Dotting Test: A Neuropsychological Screening Tool The Core Definition of the Dotting Test The dotting test stands as a remarkably straightforward, non-invasive, and cost-effective method primarily employed for the preliminary screening of various neurological diseases. At its fundamental level, this assessment requires an individual to make a series of dots on a piece of […]

The Doppelgänger Effect: Unmasking Your Mirror Image
The Doppelgänger Phenomenon Introduction to the Enigmatic Double The doppelgänger phenomenon, a concept deeply rooted in folklore and extensively explored in literature, refers to the unsettling experience where an individual perceives a seemingly identical version of themselves. This intricate psychological occurrence, also known as the doppelgänger effect or doppelgänger sighting, transcends mere superstition, presenting a […]

Domestication: The Psychology of Human Control
Domestication What is Domestication? Domestication is a profound and multifaceted process involving the modification of plants and animals from their wild forms into varieties that are more amenable to human control and beneficial for human use. This transformative process is not merely about taming individual animals or cultivating specific plants; it involves a sustained, multi-generational […]
Donders’s Law: Unlocking the Speed of Human Thought
Donders’s Law Introduction to Donders’s Law Donders’s Law stands as a foundational principle within the domain of psychophysics, a branch of psychology that investigates the relationship between physical stimuli and the sensations and perceptions they evoke. At its core, the law posits that the time required to execute a simple reaction is directly proportional to […]