
Decisional Balance: Weighing the Costs of Your Choices
Decisional Balance: A Core Concept in Health Behavior Change The Core Definition of Decisional Balance Decisional balance is a fundamental psychological construct, most notably associated with the Transtheoretical Model (TTM) of behavior change, which meticulously describes the process by which individuals contemplate and execute changes in their habits and lifestyles. At its simplest, Decisional Balance […]

Dynamic Visual Displays: Decoding Human Perception
Dynamic Visual Displays in Cognitive Psychology and Data Interpretation The Core Definition of Dynamic Visual Displays Dynamic Visual Displays (DVDs) represent a sophisticated category of data visualization tools characterized by their capacity for real-time manipulation and interaction. At its core, a dynamic visual display is a highly interactive, graphical representation of complex datasets that allows […]

Adaptive Independence: Empowering Self-Care Through Design
Assistive Technology and Independence: The Role of Dressing Aids The Core Definition of Dressing Aids Dressing aids are specialized forms of Assistive Devices specifically engineered to promote self-sufficiency in the performance of routine tasks related to dressing for individuals facing physical limitations, chronic illnesses, or temporary impairments. These tools are meticulously designed to overcome biomechanical […]
Drop-In Centers: Low-Barrier Paths to Mental Wellness
Drop-In Centers in Social and Psychological Services The Core Definition of Drop-In Centers Drop-in centers are foundational, community-based facilities designed to provide immediate, accessible, and often unconditional support services to marginalized or vulnerable populations, most notably individuals experiencing homelessness. The defining feature of a drop-in center is its low-barrier nature, meaning individuals can access vital […]
Psychological Dramatization: Why We Crave the Spotlight
Psychological Dramatization: Exaggerated Emotional Expression The Core Definition of Psychological Dramatization Psychological dramatization refers to a pervasive and habitual pattern of behavior characterized by excessive emotionality, theatricality, and a profound need to be the center of attention-seeking. It is not merely an occasional display of strong feeling, but rather a consistent style of relating to […]
Double Alternation: Mastering Patterns of Human Behavior
DOUBLE ALTERNATION The Core Definition of Double Alternation Double Alternation is defined as a systematic, non-random pattern of behavior where an individual alternates precisely between two different choices or actions on sequential, alternating occasions. Unlike simple oscillation or random choice, double alternation requires the execution of an A-B-A-B sequence, demonstrating a predictable and rule-governed structure. […]
DORA CASE: Adaptive Psychology for Rapid Service Design
DORA CASE: Data-Oriented, Rapid Adaptive, and Context-Aware Service Ecosystem The Core Definition and Scope in Applied Psychology The DORA CASE framework, standing for Data-Oriented, Rapid Adaptive, and Context-Aware Service Ecosystem, represents a sophisticated architectural approach designed to facilitate the rapid development and deployment of services capable of adapting dynamically to fluctuating user needs and environmental […]
Trisomy 21: Understanding the Psychology of Development
Down Syndrome (Trisomy 21): An Encyclopedia Entry The Core Definition and Mechanism Down Syndrome, formally known as Trisomy 21, stands as the most frequently occurring chromosomal abnormality in humans, representing a significant area of study within genetics and developmental psychology. It is fundamentally defined as a genetic disorder caused by the presence of all or […]
Dominance: Understanding the Psychology of Power
Dominance in Psychology and Behavior The Core Definition of Dominance Dominance, in the context of behavioral science and evolutionary psychology, refers fundamentally to an individual’s priority access to contested resources, often resulting from asymmetric relationships between members of the same species. It is not merely synonymous with aggression, but rather describes the established outcome of […]
Dogmatism: Why Your Brain Clings to Rigid Beliefs
Dogmatism The Core Definition of Dogmatism Dogmatism, within the field of psychology, refers to a personality trait characterized by a rigid and often unwarranted adherence to beliefs, accompanied by a profound resistance to changing those beliefs, even when confronted with compelling contradictory evidence. It represents a fundamental closed-mindedness, reflecting not the content of a person’s […]
Donepezil: Restoring Cognitive Function in Alzheimer’s
The Role of DONEPE7IL in the Treatment of Alzheimer’s Disease The Core Definition of DONEPE7IL and its Mechanism of Action DONEPE7IL is a synthetic compound developed within the realm of neuropharmacology, primarily investigated for its potential role in mitigating the symptoms and progression of Alzheimer’s disease (AD), a devastating, progressive neurodegenerative disorder. Fundamentally, DONEPE7IL is […]

Diversive Exploration: How Curiosity Drives Machine Growth
Diversive Exploration in Autonomous Systems The Core Principles of Diversive Exploration Diversive exploration is a specialized form of active learning and environmental engagement primarily utilized in the domains of robotics and artificial intelligence to enhance system autonomy. At its most fundamental level, it represents a proactive strategy where an autonomous agent deliberately seeks out novelty, […]
Disturbance of Association: Decoding Your Fragmented Mind
Disturbance of Association in Psychology The Core Definition of Disturbance of Association The concept of Disturbance of Association (DOA) refers to a fundamental disruption in the typical, expected connections between ideas, concepts, or mental representations within the cognitive system. In essence, it describes a psychological phenomenon where the normal associative link—the coherent and logical pathway […]
Cognitive Dissonance: Why Your Brain Craves Consistency
DISSONANCE REDUCTION The Core Definition of Dissonance Reduction Dissonance Reduction is a fundamental psychological process describing the mechanism by which individuals seek to minimize or eliminate the internal psychological discomfort that arises from holding two or more conflicting beliefs, attitudes, values, or behaviors. This state of conflict, formally known as Cognitive Dissonance, is experienced as […]

Cognitive Distortion: Unmasking Your Hidden Thought Traps
Cognitive Distortion The Core Definition of Cognitive Distortion Cognitive distortion is a term used in cognitive psychology and clinical psychology to describe systematic errors or biases in thinking that influence how an individual perceives reality. Essentially, a cognitive distortion represents an irrational or exaggerated thought pattern that sustains negative emotions and maladaptive behaviors, often leading […]

Disruptive Behavior Disorder: Decoding Defiance in Youth
Disruptive Behavior Disorder: An Encyclopedia Entry The Core Definition of Disruptive Behavior Disorder Disruptive Behavior Disorder (DBD) serves as an overarching category in clinical psychology, encompassing a set of psychiatric conditions characterized by chronic, persistent patterns of socially inappropriate and rule-violating behaviors. These behaviors often manifest as conflicts with authority figures, aggression toward people or […]
Disorganized Schizophrenia: Understanding the Fragmented Mind
Disorganized Schizophrenia: Clinical Characteristics, Diagnosis, and Historical Context The Core Definition and Mechanism Disorganized Schizophrenia, historically and sometimes still referred to as Hebephrenia, constitutes a severe manifestation of a chronic mental disorder characterized primarily by profound disturbances in thought processes, emotional expression, and behavior. The core mechanism distinguishing this presentation from other forms of Schizophrenia […]

Personality Disintegration: When the Self Falls Apart
Disintegration of Personality The Core Definition and Mechanism The concept of the disintegration of personality refers to a profound psychopathological state characterized by the fragmentation or breakdown of an individual’s psychic unity, resulting in a loss of cohesive identity and blurred self-boundaries. This condition, historically examined in the context of severe mental illness, posits that […]

Non-Parametric Statistics: Powerful Tools for Real Data
Distribution-Free Tests: A Comprehensive Encyclopedia Entry The Core Definition of Distribution-Free Tests A distribution-free test, commonly referred to as a non-parametric test, constitutes a critical category of statistical procedures that enable researchers to perform valid statistical inferences about a population without requiring specific assumptions regarding the precise probability distribution of the data. This approach represents […]
Schema Theory: How Your Mind Shapes Reality
Schema Theory: The Cognitive Doctrine The Core Definition of Cognitive Schemas A cognitive schema, often simply referred to as a schema theory, represents a fundamental mental structure that an individual uses to organize knowledge, interpret information, and guide behavior in the world. Essentially, a schema is a sophisticated mental framework or blueprint that encapsulates a […]
Divergent Thinking: Unlock Your Creative Potential
Divergent Production: A Psychological and Organizational Review The Core Psychological Definition Divergent production, often referred to as Divergent Thinking, is a cognitive process used to generate creative ideas by exploring many possible solutions. It stands in contrast to convergent thinking, which focuses on finding a single, correct answer. This process is fundamental to the study […]

Dissociative Patterns: Unlocking the Science of Disconnection
The Dissociative Pattern in Psychology The Core Definition of Dissociation The dissociative pattern is a complex psychological phenomenon characterized by a fundamental disruption or discontinuity in the normal integration of consciousness, memory, identity, emotion, perception, body representation, and motor control. At its simplest, dissociation represents a disconnection—a mental mechanism where the mind separates threatening or […]

Distorted Speech: Decoding Language Under Pressure
Distorted Speech Test The Core Definition of the Distorted Speech Test The Distorted Speech Test (DST) is a specialized psycholinguistic tool meticulously designed to evaluate an individual’s ability to process and understand spoken language under conditions of acoustic stress. At its core, the DST assesses individual differences in speech perception by utilizing meticulously manipulated speech […]

Display-Control Compatibility: Design for Intuitive Minds
Display-Control Compatibility The Core Definition of Display-Control Compatibility Display-Control Compatibility, often abbreviated as DCC, is a fundamental principle within Human-Computer Interaction (HCI) and Human Factors Psychology. It refers to the degree to which the arrangement, movement, and operation of a control device logically corresponds to the resulting movement, change, or presentation on its associated display […]

Developmental Levels: Mapping Your Growth Journey
DEVELOPMENTAL LEVELS The Core Concept: Defining Developmental Levels The concept of Developmental Levels refers to the structured progression through which human beings acquire increasingly complex physical, cognitive, emotional, and social capacities across the lifespan. It is based on the fundamental idea that individuals do not change randomly but rather move sequentially through identifiable developmental stages, […]
Deoxycorticosterone: The Stress Hormone That Shapes Mood
Deoxycorticosterone: A Key Mineralocorticoid Precursor Core Definition and Physiological Role Deoxycorticosterone, often abbreviated as DOC, is a crucial steroid hormone produced primarily by the adrenal cortex. Chemically, it is classified as a mineralocorticoid, although it serves predominantly as a potent precursor, or prohormone, in the metabolic pathway leading to the synthesis of aldosterone, the body’s […]
Dendrophilia: Why We Form Deep Bonds With Nature
Dendrophilia: The Human Emotional Connection to Trees Defining Dendrophilia: The Core Concept Dendrophilia is a specialized psychological and anthropological term used to describe a profound, often emotional or spiritual, affinity and connection between humans and trees. At its simplest, it represents the love of trees and forests. This concept moves beyond mere appreciation of natural […]
Psychological Detox: Clearing Mental Clutter for Clarity
Detoxification: Biological Mechanisms and Behavioral Context The Core Definition of Biological Detoxification Detoxification is fundamentally defined as the complex, natural, physiological process by which living organisms neutralize, transform, and eliminate unwanted chemical compounds, often referred to as toxins or metabolic waste products. This essential biological function, sometimes casually referred to as detoxing or toxic elimination, […]
Cognitive Dissonance: Why Your Brain Hates Contradictions
Cognitive Dissonance Theory The Core Definition of Cognitive Dissonance The psychological phenomenon known as Cognitive Dissonance refers to the profound mental stress or discomfort experienced by an individual who simultaneously holds two or more contradictory beliefs, ideas, or values. This conflict, which is often emotionally and psychologically taxing, arises when an individual’s actions are inconsistent […]

Responsive Parenting: Balancing Needs and Autonomy
Demand Feeding and Self-Denial in Parenting Psychology Introduction and Core Definitions Demand feeding and self-denial represent two fundamentally distinct philosophies regarding responsive parenting and the establishment of autonomy in early childhood, particularly concerning nutritional intake and emotional responsiveness. While both are concerned with shaping a child’s relationship with their needs and desires, they employ contrasting […]


Delay-of-Reward: Why Waiting Feels So Difficult
documentclass{article} usepackage{apacite} begin{document} title{The Delay-of-Reward Gradient Effect: A Review} author{John Doe} maketitle begin{abstract} The delay-of-reward gradient (DORG) is an effect observed in studies of reward-based behaviors in humans and animals. This review article explores the theoretical and empirical evidence for the DORG effect, its implications, and future directions of research. We summarize the current literature, […]
The Decline Effect: Why Your Favorite Studies Fail
DECLINE EFFECT The Core Definition of the Decline Effect The Decline Effect refers to a widespread phenomenon observed across various scientific disciplines, including psychology, where the magnitude of a measured effect or finding tends to decrease significantly when studies are repeated or replicated over time. Initially promising results, often published with a large effect size […]
Defective Delinquency: Unmasking the Roots of Criminality
Defective Delinquency The Core Definition of Defective Delinquency Defective delinquency is a specialized term in forensic and clinical psychology used to denote delinquent behavior that is understood to be the direct result of an underlying mental health disorder, cognitive impairment, or neurodevelopmental deficit. At its core, this concept serves as a critical distinction, shifting the […]

Deficiency Love: Why We Seek Completion in Others
Deficiency Love (D-Love) in Psychology The Core Definition of Deficiency Love (D-Love) Deficiency Love, commonly abbreviated as D-Love, is a theoretical construct coined within the framework of humanistic psychology, primarily associated with the work of Abraham Maslow. At its simplest, D-Love is a form of love or attachment that arises from the psychological need to […]
Cognitive Defense: Mastering the Art of Dehoaxing
Dehoaxing: A Framework to Detect and Mitigate Fake News Fake news has become a major threat to democracies across the world. The proliferation of false information has resulted in the erosion of public trust, the propagation of misinformation, and the manipulation of public opinion. In response, numerous approaches have been developed to detect and mitigate […]

DEJA VU
Deja Vu: An Overview of the Phenomenon Deja vu is a French expression for “already seen” that is used to describe the feeling of familiarity one experiences when experiencing something for the first time (Hirshorn, 2018). It is a phenomenon that has been reported by approximately two-thirds of the population in the United States. This […]

Deductive Reasoning: Mastering the Logic of the Mind
Deductive reasoning, also known as logical deduction, is a type of logical argument in which a conclusion is drawn from two or more premises that are generally assumed to be true. The premises in a deductive argument are typically statements that are assumed to be true, while the conclusion is intended to be a logically […]

Dyssocial Personality: Decoding the Roots of Callousness
Dyssocial Personality: An Encyclopedia Entry The Core Definition of Dyssocial Personality Dyssocial personality refers to a specific type of personality disorder characterized by a pervasive pattern of grand selfishness, profound callousness, and a fundamental disregard for the feelings, rights, and safety of others. This definition, often utilized within European diagnostic frameworks such as the International […]

Distance Vision: Mastering How We Perceive the World
Distance Vision: An Encyclopedia Entry The Core Mechanisms of Distance Vision The ability to perceive objects clearly and accurately across significant spatial separation is formally defined as Distance Vision. This fundamental visual skill is essential for effective human interaction with the environment, enabling navigation, hazard anticipation, and the recognition of objects far beyond arm’s reach. […]
Distributed Representation: Mapping the Human Mind
Distributed Representation is a type of representation used in machine learning that encodes knowledge in a neural network as a set of real-valued vectors. It is an important component of deep learning and is used to represent words, phrases, and other types of text in a way that allows for automatic performance of tasks such […]

Deceptive Advertising: How Brands Trick Your Brain
Deceptive Advertising: A Psychological and Legal Analysis The Core Definition of Deceptive Advertising Deceptive advertising is fundamentally defined as the intentional use of false, misleading, or unsubstantiated claims in commercial communications designed to induce consumers into purchasing an advertised product or service. This practice transcends mere puffery—the legal term for subjective, exaggerated claims that no […]
Cognitive Dissonance: The Mental Tug-of-War Within You
Cognitive Dissonance Theory The Core Definition and Fundamental Mechanism Cognitive Dissonance is a foundational concept in social psychology, defined as the state of psychological discomfort or tension experienced when an individual simultaneously holds two or more conflicting cognitions (ideas, beliefs, values, or emotions) or when their actions contradict their beliefs. This internal conflict creates an […]
DIRECTOR Model: Mastering Your Internal Cognitive Monitor
The DIRECTOR Model of Cognitive Oversight The Core Definition: Conceptualizing the Internal Monitor The DIRECTOR model, standing for Directed Internal Regulatory Oversight, posits a specialized Cognitive Mechanism responsible for actively monitoring, analyzing, and adjusting an individual’s internal stream of thought, emotional response data, and subsequent behavioral output. Essentially, DIRECTOR functions as the mind’s built-in supervisory […]
Mentorship: The Psychology of Deep Personal Growth
Disciple Making: A Comprehensive Encyclopedia Entry The Core Definition of Disciple Making Disciple Making is fundamentally understood within Christian theology as a process of intentional and purposeful discipleship designed to foster profound spiritual growth and transformation in individuals. At its simplest, it is the ongoing effort to guide another person into becoming a dedicated follower […]
Dimerization: The Psychology of Social Bonding
Dimerization: Molecular Principles and Biological Significance The Core Definition of Dimerization Dimerization, fundamentally defined within the realm of molecular biology and biochemistry, is the precise chemical reaction in which two individual molecular units, often referred to as monomers, combine to form a single, larger molecular complex known as a dimer. This process is highly crucial […]

Facial Action Studies: Decoding Human Emotion Through Movement
DIRECTED FACIAL ACTION STUDIES Introduction and Core Definition Directed Facial Action Studies (DFAS) represent a specialized and powerful methodology within affective science designed to investigate the complex relationship between facial musculature, physiological response, and subjective emotional experience. At its core, DFAS involves instructing research participants to volitionally contract specific facial muscles—often referred to by their […]
Levels of Processing: How Deeper Thinking Boosts Memory
Levels of Processing Theory: An Overview The Core Definition of Levels of Processing The Levels of Processing (LOP) theory, a fundamental framework within cognitive psychology, posits that the depth at which information is processed during encoding determines the durability and strength of the resulting memory trace. Unlike earlier models that focused on fixed structural components […]
Cognitive Dissonance: Master Your Inner Conflict
Cognitive Dissonance The Core Definition of Cognitive Dissonance Cognitive Dissonance is fundamentally the mental stress or discomfort experienced by an individual who holds two or more contradictory beliefs, ideas, or values, or is confronted by new information that conflicts with existing beliefs, attitudes, or behaviors. At its simplest, it is a state of internal inconsistency […]
Einstellung: How Your Mental Set Shapes Every Choice
Determining Tendency (Einstellung) The Core Definition of Determining Tendency The concept of Determining Tendency, derived from the German term Einstellung, is a foundational principle in early experimental and cognitive psychology, defining an unconscious preparatory state or predisposition that directs an individual’s cognitive processes toward a specific goal or outcome. This psychological “set” acts as an […]

Desurgency: A Behavioral Shift in Emergency Response
Desurgency: A Behavioral Approach to Emergency Medical Services The Core Definition of Desurgency Desurgency represents a modern, proactive methodological shift in the delivery of emergency medical services (EMS), fundamentally redefining the traditional response model. At its most concise, desurgency refers to the strategic provision of timely and appropriate medical interventions to patients who are assessed […]
Cognitive Dissonance: Why Your Brain Hates Contradictions
Cognitive Dissonance Theory The Core Definition and Mechanism Cognitive Dissonance is a fundamental and widely studied psychological phenomenon defined as the state of mental discomfort experienced by an individual who simultaneously holds two or more contradictory cognitions, such as beliefs, values, or attitudes, or when their behavior contradicts one of their existing beliefs. This psychological […]

Human Development: Mastering Your Personal Life Cycle
The Software Development Life Cycle (SDLC) The Core Definition and Mechanism The Software Development Life Cycle (SDLC) is a crucial framework used in Software Engineering that defines a structured sequence of stages for planning, creating, testing, and deploying an information system or software application. It serves as a methodology for improving the quality of software […]
Psychosocial Dwarfism: When Stress Stunts Growth
Deprivation Dwarfism: Psychosocial and Endocrine Perspectives The Core Definition: Understanding Deprivation Dwarfism Deprivation dwarfism, clinically referred to as Psychosocial Short Stature (PSS) or Psychosocial Dwarfism, is a severe growth disorder characterized by significantly reduced physical growth and maturity that is not attributable to primary nutritional deficiencies, genetic disorders, or known organic disease. Instead, the condition […]
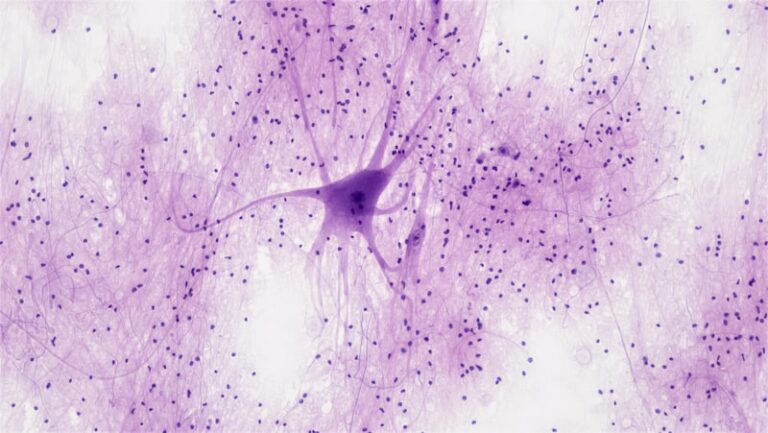
Dendrodendritic Synapses: How Neurons Talk to Each Other
The Dendrodendritic Synapse: Structure, Function, and Significance The Core Definition and Mechanism The dendrodendritic synapse represents a highly specialized and unique form of connection within the central nervous system, fundamentally defined by the direct point of contact between the dendrite of one neuron and the dendrite of another neuron. Unlike the vast majority of neuronal […]
Psychological Derangement: Understanding Mental Chaos
Derangement in Clinical Psychology Introduction: Defining Psychological Derangement The term Derangement, while largely considered an antiquated term in contemporary psychiatry, describes a profound and comprehensive disturbance of the mental faculties, suggesting a state where the normal organization and function of the mind have become fundamentally disordered. Historically, it served as a broad classification for severe […]
Depersonalization: Understanding the Self-Detachment Gap
Depersonification: Definition, Experience, and Clinical Context The Core Definition of Depersonification Depersonification, often studied clinically under the umbrella term depersonalization, is fundamentally defined as a psychological process wherein an individual experiences a profound sense of detachment or alienation from their own self. This core experience transcends mere introspection or momentary reflection; it involves perceiving oneself, […]
Logical Fallacies: Mastering the Art of Clear Thinking
Denying the Consequent: A Formal Fallacy The Core Definition of Denying the Consequent Denying the Consequent is a term rooted in conditional statements, which are fundamental building blocks of both philosophical and psychological approaches to deductive reasoning. In formal logic, the phrase “Denying the Consequent” refers to a valid inference rule known as Modus Tollens. […]
The Delta Rule: How Minds Master Learning Through Error
The Delta Rule in Computational Psychology The Core Definition and Mechanism of the Delta Rule The Delta Rule, often recognized synonymously as the Widrow-Hoff Rule or the Least Mean Squares (LMS) algorithm, constitutes a foundational principle in the realm of connectionist modeling and computational learning theory. At its core, the Delta Rule is a powerful […]

Déjà Vu: Why Your Brain Triggers False Memories
Déjà Vu: A Phenomenological and Cognitive Analysis The Core Definition of Déjà Vu Déjà Vu (DV) is fundamentally defined as a compelling, yet often transient and unsettling, subjective experience of recognizing a present moment or situation as having been encountered or lived through previously, even though the individual retains no conscious, explicit recollection of the […]

Speech Delay: Unlocking Your Child’s Hidden Potential
Delayed Speech: An Encyclopedia Entry The Core Definition of Delayed Speech Delayed speech, often categorized clinically under the broader umbrella of language development disorders, refers specifically to a delay in the production and articulation of spoken sounds, words, and sentences beyond the typical developmental milestones expected for a child’s chronological age. While language delay encompasses […]
Demand Characteristics: Why Your Study Might Be Biased
Demand Characteristics The Core Definition of Demand Characteristics Demand characteristics represent a critical form of experimental artifact in psychological research, fundamentally threatening the internal validity of findings. Broadly defined, a demand characteristic is any subtle cue or set of cues that inadvertently communicates the purpose of the experiment or the expected behavioral response to the […]
Demographic Psychology: How Population Shapes Your Mind
Demography and its Psychological Implications The Core Definition of Demography Demography is fundamentally the systematic and statistical study of human populations, focusing intently on their size, structure, distribution, and the continuous processes that cause changes in these characteristics over time. The core mechanism driving demographic analysis relies on three primary variables: births (fertility), deaths (mortality), […]
Degrees of Freedom: Unlocking Statistical Precision
DEGREES OF FREEDOM PROBLEM The Core Definition in Quantitative Psychology The Degrees of Freedom (DF) problem is a fundamental challenge encountered in quantitative methods, particularly within Linear Models and sophisticated statistical analyses widely utilized in psychological research. Fundamentally, the DF concept refers to the number of values in the final calculation of a statistic that […]

Nutrient Deficiency: How Hidden Hunger Impacts Your Mind
DEFICIENCY The Core Definition of Nutrient Deficiency The concept of Nutrient Deficiency, often referred to as undernutrition or specifically micronutrient deficiency, describes a state where the body lacks sufficient quantities of one or more essential vitamins or minerals required for optimal physiological function. This condition is far more than simply feeling unwell; it represents a […]
Deep Processing: Elevate Your Cognitive Efficiency
DEEP PROCESSING Introduction: The Core Definition The concept of Deep Processing, within the context of modern computational psychology and artificial intelligence, refers to an advanced technique that systematically integrates principles derived from Cognitive Science with sophisticated Machine Learning methodologies. This hybrid approach is specifically designed and implemented to enhance and optimize traditional cognitive functions such […]
Defect Theory: Decoding the Roots of Mental Dysfunction
Defect Theory in Psychological Modeling 1. The Core Definition of Psychological Defect Theory Defect Theory, when applied within the field of psychopathology, posits that certain psychological disorders or behavioral dysfunctions arise primarily from inherent, structural, or biological imperfections within the individual’s neural architecture or cognitive machinery. Unlike models focusing on purely environmental conditioning or transient […]

Declarative Memory: Unlock Your Mind’s Mental Library
Declarative Memory The Core Definition of Declarative Memory Declarative memory, often referred to as explicit memory, is a major subsystem of long-term memory dedicated to storing information that can be consciously recalled and explicitly stated or “declared.” This form of memory encompasses facts, concepts, and specific events associated with particular contexts. Unlike non-declarative or implicit […]

Diagnostic Interview: Unlocking the Path to Mental Clarity
Diagnostic Interview The Core Definition and Mechanism The Diagnostic Interview serves as the foundational, systematic method utilized by mental health professionals—including psychiatrists, psychologists, and clinical social workers—to gather comprehensive information from a client or patient. This process is essential for evaluating symptoms, understanding the client’s history, and ultimately formulating a formal diagnostic hypothesis concerning potential […]
Deductive Reasoning: Master the Art of Logical Certainty
Deductive Reasoning The Core Definition of Deductive Reasoning Deductive Reasoning, often simply called deduction, is a fundamental logical process wherein reasoning proceeds from one or more general statements, known as premises, to reach a logically certain conclusion. It is a form of inference where the conclusion is necessarily true if the premises are true. The […]

The Diaphragm: The Hidden Anchor of Emotional Calm
The Diaphragm: Anatomy and Function in Respiration and Psychophysiology The Core Definition and Muscular Structure The diaphragm is fundamentally defined as the primary, large sheet of skeletal muscle that horizontally separates the human thoracic cavity, which houses the heart and lungs, from the abdominal cavity below, which contains the digestive organs. This anatomical separation is […]
Deconditioning: Breaking the Cycle of Mental and Physical Stagnation
Deconditioning: A Biopsychosocial Perspective The Core Definition of Deconditioning Deconditioning, fundamentally, refers to the physiological and psychological changes that occur in an individual following a period of sustained physical inactivity, often resulting in a noticeable decline in physical fitness, functional capacity, and overall health. While the term is frequently utilized within physical therapy and rehabilitation […]

Persistent Depressive Disorder: Finding Light in the Grey
DYSTHYMIC DISORDER (Persistent Depressive Disorder) The Core Definition and Fundamental Mechanism The psychological condition formerly known as Dysthymic Disorder, and now classified in the DSM-5 as Persistent Depressive Disorder (PDD), represents a chronic, long-term form of depression characterized by persistent low mood and general unhappiness that lasts for a minimum of two years in adults […]
Decision Rules: Mastering Your Choices Under Uncertainty
Decision Rules in Psychology and Cognition The Core Definition of Decision Rules Decision rules, at their core, are systematic procedures or explicit guidelines designed to facilitate the selection of an optimal course of action from a set of available alternatives, particularly when facing conditions marked by inherent risk or uncertainty. These rules provide a structured […]

Dysphoria: Navigating the Depths of Emotional Unease
DYSPHORIA Introduction: Understanding Dysphoria Dysphoria is a complex and often debilitating psychological state characterized by a pervasive sense of unease, dissatisfaction, or profound unhappiness. It extends beyond transient sadness or disappointment, representing a more enduring and generalized feeling of emotional discomfort that significantly impacts an individual’s perception of life and well-being. This state is not […]
Dysmnesia: Unlocking the Mysteries of Fragmented Memory
DYSMNESIA Introduction to Dysmnesia Dysmnesia represents a specific category of memory disorders characterized by considerable difficulty in recalling previously stored memories or facts. Unlike some forms of amnesia which might involve the complete loss of memory for certain periods, dysmnesia primarily pertains to the impaired retrieval of accessible information. This condition does not necessarily imply […]

Pain Management: The Psychology of Chronic Relief
DURAGESIC: A Comprehensive Overview The Core Definition of DURAGESIC DURAGESIC, known generically as the fentanyl transdermal system, is a specialized medication delivery method designed for the sustained management of chronic, severe pain in adult patients who require continuous opioid analgesia and who are already opioid-tolerant. It constitutes a discreet patch applied directly to the skin, […]
Dysexecutive Syndrome: Mastering Your Brain’s Control Center
Dysexecutive Syndrome (DES) Introduction: Understanding Dysexecutive Syndrome (DES) Dysexecutive Syndrome (DES) is a complex neurological and psychological disorder characterized by significant impairments in a collection of higher-order cognitive processes known as executive functions. These functions are crucial for goal-directed behavior, problem-solving, and adapting to new situations. Essentially, DES represents a breakdown in the brain’s “command […]

Drug-Induced Psychosis: Understanding the Mind’s Break
Drug-Induced Psychosis The Core Definition of Drug-Induced Psychosis Drug-induced psychosis (DIP) is a severe, yet often reversible, mental health condition characterized by the sudden onset of psychotic symptoms directly attributable to the use of, or withdrawal from, psychoactive substances. This condition manifests primarily through disturbances in thought, perception, and emotion, leading to a significant disconnect […]

Haptic Communication: The Hidden Language of Human Connection
Dynamic Touch Introduction: The Profound Language of Touch Touch stands as one of the most fundamental and pervasive forms of human interaction, a primal sense that shapes our perceptions of the world and our relationships with others. Far more than a mere physical sensation, touch communicates a vast spectrum of information, from comfort and intimacy […]

DYNAMIC
Dynamic Processes in Psychology Introduction to Dynamic Processes in Psychology In the realm of psychology, the term dynamic refers to processes, systems, or interactions characterized by continuous change, activity, and evolution over time. Unlike static views that perceive mental states or behaviors as fixed entities, a dynamic perspective emphasizes the constant flux, interaction, and transformation […]

Dual-Aspect Physicalism: Bridging Mind and Matter
Dual-Aspect Physicalism The Core Definition of Dual-Aspect Physicalism Dual-aspect physicalism is a sophisticated philosophical position within metaphysics that endeavors to bridge the traditional chasm between physicalism and dualism. At its heart, it posits that while reality is fundamentally physical, this physical reality inherently possesses two inseparable aspects: a physical aspect, which is publicly observable and […]

Driver Psychology: Mastering the Mind Behind the Wheel
Driver Training Core Definition of Driver Training Driver training, often interchangeably referred to as driver education, constitutes a structured program designed to instruct individuals in the theory and practical aspects of operating a motor vehicle safely and responsibly. It encompasses a comprehensive curriculum that goes beyond mere mechanical operation, focusing instead on cultivating a deep […]

Dream Stimulus: How External Cues Shape Your Nightly Reality
Dream Stimulus: A Review of Neurophysiological Findings Abstract Dreams are a complex neurophysiological phenomenon in which mental images, emotions, and sensations are experienced during sleep. The role of external stimuli in the formation of dreams has been studied extensively, and research suggests that dream stimuli can alter dream content. This review outlines current knowledge of […]